Policy view: worldwide patterns of tobacco use with recommendations for tobacco control

Fourth paper in a Lancet Respiratory Medicine Series on the global epidemiology of chronic respiratory disease.
Key messages
- The tobacco industry caused more than 200 million deaths over the past 30 years, with 7.4 million in 2023 alone. The commercial tobacco epidemic remains a leading cause of preventable respiratory diseases — approximately 30% of deaths from chronic obstructive pulmonary disease and half of all lung cancer deaths, with many countries now seeing lung cancer mortality among women surpass breast cancer rates.
- The current global situation shows that there are opportunities to act and save lives. If urgent action is taken now, incipient tobacco epidemics in countries with low tobacco use can be quashed and growing epidemics minimised much more rapidly. In countries with high male tobacco use prevalence, fast implementation of new measures and better enforcement of existing measures can often still avert a rise in tobacco use among women, which remains low in many regions.
- The rise of new nicotine products (such as e-cigarettes) and new tobacco products (such as heated tobacco products) presents new challenges. These products are often targeted at young people and, if widely available, can result in elevated population-level nicotine use and increased harm. The potential for ENDS to act as a gateway to tobacco use among young people is particularly concerning — it could reverse progress in countries that have successfully reduced tobacco use prevalence from previously high levels.
- The WHO FCTC and the measures of the MPOWER technical package have been indispensable in reducing tobacco use and tobacco use prevalence globally. These resources provide a proven set of commitments and implementation framework for addressing the commercial tobacco epidemic and the threats posed by new and emerging products.
- Funding limitations and industry interference remain principal barriers to progress. Adoption and enforcement of the WHO FCTC and related MPOWER measures remains inconsistent across countries, leaving 2.3 billion people without protection from even one measure at a best-practice level of implementation.
Introduction
The tobacco industry depends on maximising tobacco sales for its financial health and survival. Tobacco is health-harming: it is highly addictive and toxic both to the people who use it and, when smoked, also to others in the vicinity. The inherently toxic tobacco plant became an epidemic-level threat when the tobacco industry turned it into a mass-consumer product at the turn of the 20th century, by altering the flavour and harshness of tobacco smoke to make it more palatable, changing the way it is consumed for improved convenience, and using advertising and other marketing practices to cultivate population-wide demand. The tobacco industry’s products are some of the leading risk factors for the development of the major non-communicable diseases (NCDs) that together account for approximately half of all global mortality. Lung cancer and chronic respiratory diseases feature prominently among these NCDs.
Over more than a century, as a large-scale commercial operation, the tobacco industry has become a leader and pioneer in the business of reaping profit while causing death, disease and suffering. It caused 100 million deaths in the 20th century and more than 200 million in the past thirty years. In 2023 alone, it caused 7.4 million deaths — more than 12% of total global mortality. If current trends continue, the cost to humanity of the industry’s drive for private profit is estimated to amount to more than a billion deaths in this century.
The tobacco industry has also proven effective at externalising the costs of its business model onto countries, communities and families worldwide. The annual economic cost of smoking-attributable diseases has been estimated at more than US$ 1436 billion, equivalent to 1.8% of the world’s annual GDP. This includes health-care expenditures of US$ 422 billion on smoking-attributable disease and indirect economic costs of US$ 1014 billion from productivity losses due to the health conditions and premature mortality caused by tobacco-related disease. Almost 40% of these total economic and income losses now occurs in low-income and middle-income countries. If the tobacco industry was made to pay for the full scale of these costs, it would no longer be in business.
Despite these immense harms, the tobacco industry has successfully shielded itself from comprehensive public health responses and continues to aggressively market its deadly product. As a result, approximately 20.9% of the global population aged 15 years and older were still using some form of tobacco in 2022, and the costs of tobacco-related disease are continuing to rise. Therefore, the abated but not averted commercial epidemic of tobacco-related disease remains a defining global health problem for the 21st century. It continues because of the power the industry still has to shape our politics, knowledge and beliefs in ways that protect its profit from measures that would protect and promote health. Indeed, the health threat from tobacco became apparent by the 1950s and, by the 1980s, a strong evidence base had developed on the measures needed in response. Yet in 2025, more than 40 years after both the problem and effective resolutions were substantiated, the world remains far short of comprehensive tobacco control. As such, the tobacco industry, its power and the ways in which it interferes in politics and science remain the pre-eminent obstacle to progress.
In response to this global epidemic, the WHO Framework Convention on Tobacco Control (WHO FCTC) was adopted by unanimity at the World Health Assembly in 2003 and entered into force in February 2005. With 183 Parties, the WHO FCTC encompasses more than 90% of the world’s population and constitutes a unifying framework for action at the national level and for intergovernmental cooperation in countering tobacco industry tactics and combatting the tobacco epidemic. This legally binding treaty comprises a core set of demand- and supply-reduction obligations, supported by general obligations to prevent industry interference in public health policy and advance progress and cooperation on tobacco control at local, national, regional and global levels.
The Conference of the Parties — the governing body to the WHO FCTC — has adopted guidelines for the implementation of the main demand-reduction articles. To support full implementation, WHO also developed a technical package (the MPOWER package) containing the main demand-reduction measures, which were also recommended as WHO best buys for the prevention and control of NCDs. All the measures contained in the WHO FCTC in general, and in MPOWER in particular, are evidence-based, highly effective, mutually reinforcing, and best implemented in a comprehensive manner.
The priority of the tobacco control response in global health can be seen in its importance to achieving UN Sustainable Development Goal (SDG) 3.4 — to reduce premature mortality from NCDs by one-third by 2030. The WHO FCTC is explicitly referenced under Goal 3, with target 3.a calling for countries to strengthen implementation. Because of the broad economic and environmental costs of tobacco, WHO FCTC measures also support several other SDGs, including economic growth, poverty reduction and the creation of healthy environments.
The WHO FCTC has been instrumental in curbing the global tobacco epidemic, with tobacco use prevalence steadily decreasing and projections indicating a continued decline in the absolute number of people using tobacco. However, progress has been insufficient, with the implementation of the treaty’s provisions varying across different articles and Parties. The under-implementation and under-enforcement of the WHO FCTC’s provisions is a result of the power that the well-resourced and well-organised tobacco industry has to deter, prevent, delay and undermine progress.
Tobacco use trends
Evolution of the tobacco epidemic
Globally, the number of people who use tobacco peaked in 2010, and tobacco use prevalence has steadily declined over the last two decades. This headline, however, obscures important shifts in the distribution of tobacco use — with substantial decreases in many countries with advanced epidemics accompanied by slow progress or even increases in others, alongside variations between women and men and among socioeconomic and demographic groups across all countries.
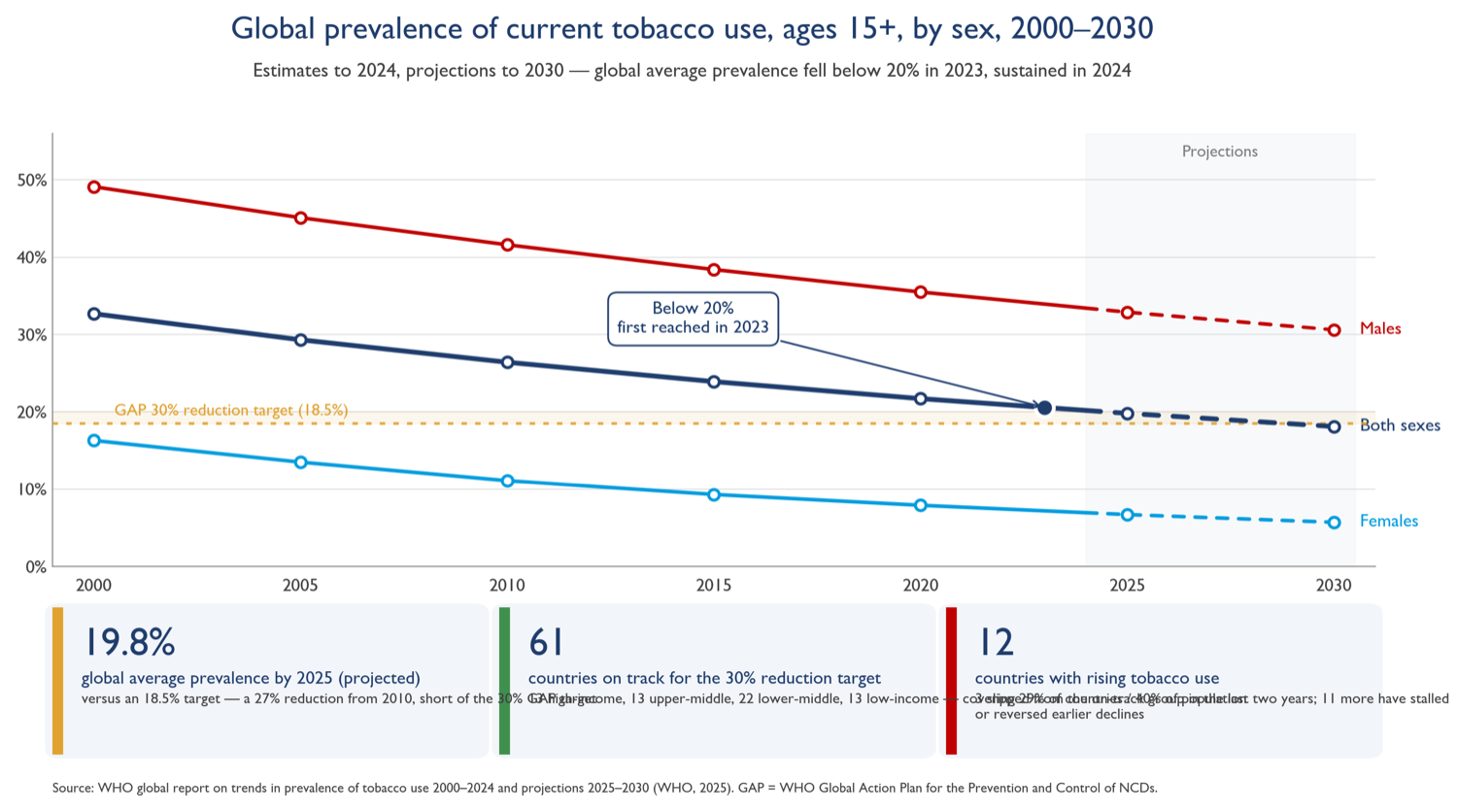
Figure 1 (redrawn): global prevalence of current tobacco use, ages 15+, by sex, 2000–2030. Source: WHO global report on trends in prevalence of tobacco use.
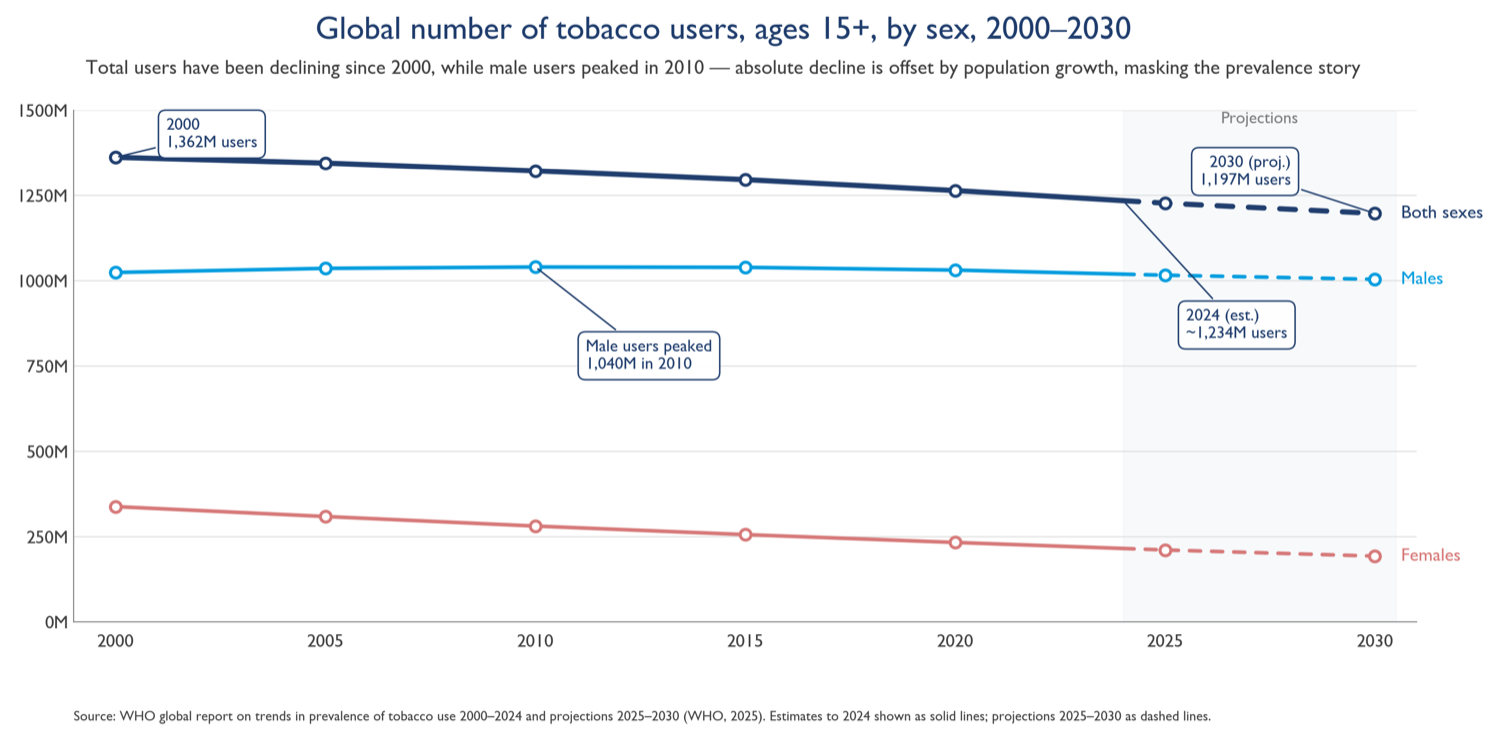
Figure 2 (redrawn): global number of tobacco users, ages 15+, by sex, 2000–2030. Source: WHO.
These differences can be understood according to stages that describe the way in which the tobacco epidemic tends to unfold across countries and population groups: socioeconomic factors and tobacco industry market practices increase tobacco use from a first-stage incipient epidemic to a second-stage escalating epidemic; increasing tobacco-related burden and increased awareness of these harms tends to trigger a commensurate response in the form of public health measures, resulting in a third stage of initial declines but still high prevalence. With more ambitious tobacco control, prevalence can decrease to less than 25% in the fourth stage.
Understanding how tobacco epidemics within countries tend to evolve according to stages also means understanding that they tend to evolve distinctly according to sex. Attention needs to be paid to the particularities of tobacco epidemics in women. In most cases, peak smoking prevalence among women has never reached the peak levels among men. Changes in the increase and decrease of smoking prevalence among women generally lag behind men by two or three decades, especially in high-income and upper middle-income countries. Therefore, rapid action in countries with high tobacco use prevalence among men can often still avert a rise in tobacco use among women, which remains low in many regions.
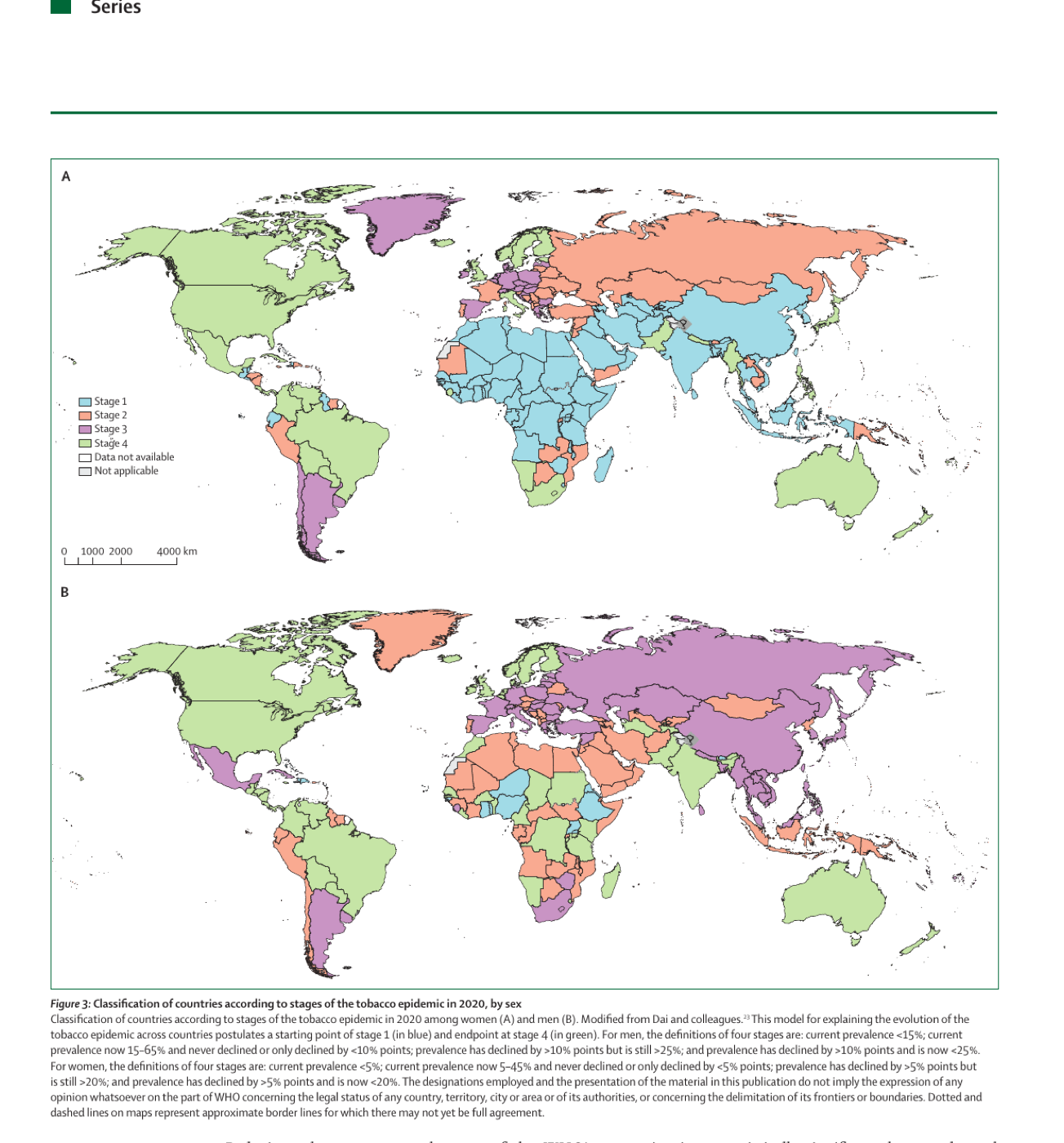
Figure 3 (reproduced from the paper): classification of countries according to stages of the tobacco epidemic in 2020, by sex (A: women; B: men).
This model is not immutable, and the implementation of comprehensive tobacco control measures affects it. By no means is it a destiny for countries with low tobacco use prevalence to transit through the four stages — if urgent action is taken, incipient epidemics can be quashed and growing epidemics can be slowed and reversed much more rapidly than has been possible in the past. At the same time, there is no reason for complacency among countries in the third or fourth stage. The trajectory predicted in the model can be subverted: for example, the potential for electronic nicotine delivery systems (ENDS) to act as a gateway to tobacco use among young people is concerning, as it could undermine progress made in reducing smoking rates within countries with advanced epidemics and now low tobacco use prevalence.
Urgent action is therefore needed to quash the epidemics in countries with incipient epidemics and among women: action to halt epidemics before they escalate, bend the curve in rising epidemics and maintain progress everywhere. Despite some progress, many countries are not on track to meet the SDG 3.4 target and the world as a whole is not on track to reduce premature mortality from NCDs by the amount declared in the commitment. Based on 2010–2016 data, women in 17 (9.7%) of 176 countries and men in 15 (8.5%) of 176 countries are expected to achieve SDG target 3.4. Among high-income countries, men and women in Denmark, Luxembourg, New Zealand, Norway, Singapore and South Korea are on track to meet the target if they maintain or surpass their 2010–2016 average rate of decline in NCD-related mortalities.
Reducing tobacco use was also part of the WHO’s nine voluntary targets to combat NCDs by 2025. WHO reported in 2024 that 56 countries were likely to have achieved at least a 30% relative reduction in tobacco use by 2025, assuming they could continue to implement tobacco control measures at their previous pace or faster. Another 94 countries were experiencing a statistically significant downward trend but were considered unlikely to have achieved the target in 2025 in the absence of acceleration of efforts. The 56 countries currently on track to meet the reduction target represent 29% of the world’s countries and 40% of the world’s population. But compared with the 2022 assessment, there has been a net loss of four countries.
The product landscape
Although conventional tobacco products continue to dominate, the market has seen a proliferation of new nicotine products (including ENDS such as e-cigarettes) and new tobacco products (such as heated tobacco products — HTPs). Alongside HTPs, ENDS are generally marketed indiscriminately to all people but particularly to young people. These products are often portrayed as cessation aids and healthier alternatives to conventional cigarettes. Although the industry officially presents them as an alternative for people who smoke, in reality a major share of their marketing efforts target young people — including through social media, with the help of influencers, and through the development of products with youth appeal such as e-cigarettes with various flavours and sleek designs. The risks posed by the products are exacerbated and magnified by the tobacco industry’s efforts to obscure the difference between these two distinct product categories. This strategy enables producers of HTPs — which are clearly tobacco products — to claim their products are similar to ENDS and classify them together with ENDS in a way that supports efforts to both lobby policymakers for favourable treatment and shape consumer perception of the product category.
Across 97 countries, conventional cigarettes still account for the overwhelming majority of tobacco and nicotine retail value, but the retail value and market share of new and emerging products — e-cigarettes and heated tobacco products in particular — have grown steadily since 2007 (figure 4).
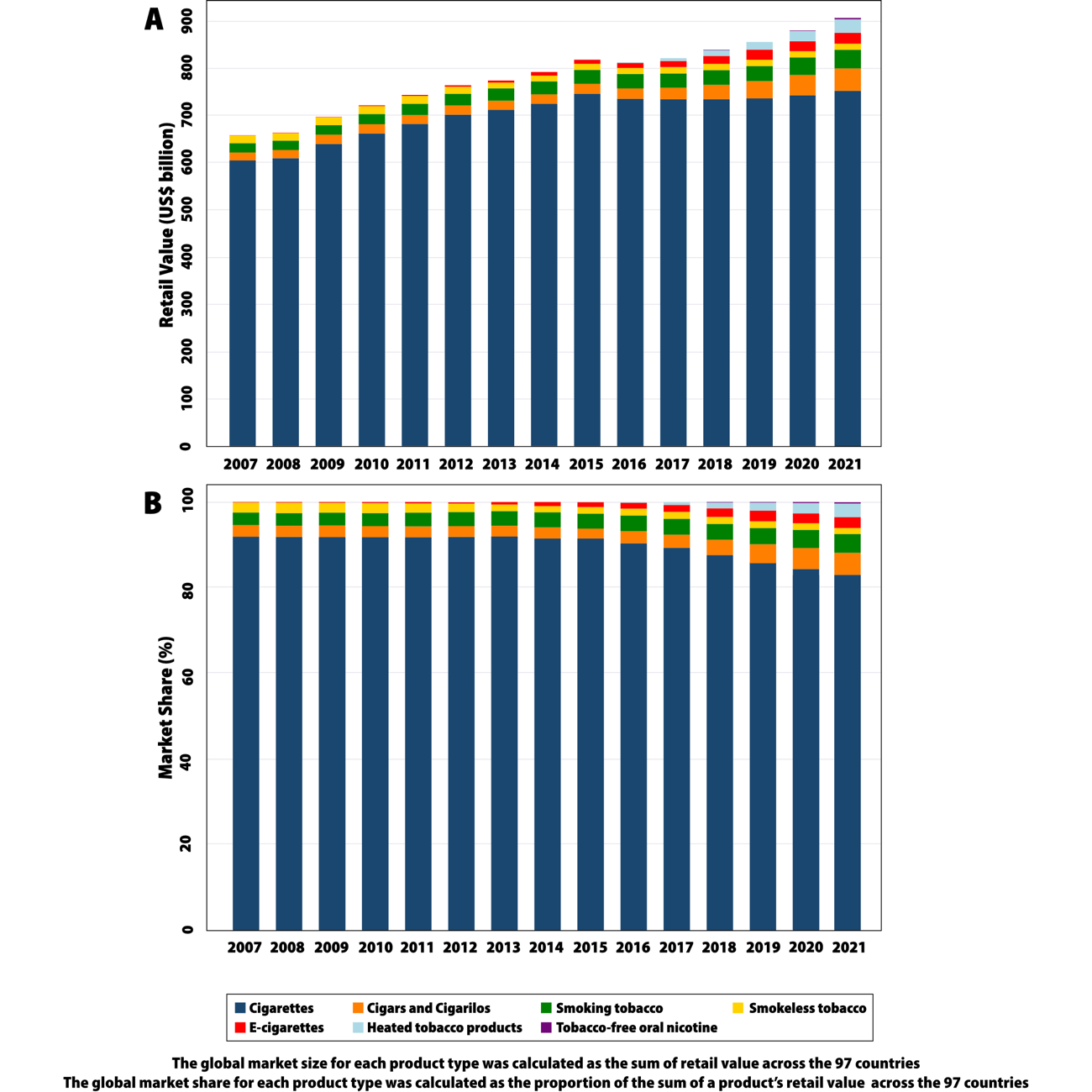
Figure 4: the global tobacco and nicotine product landscape, 2007–2021 — retail value (panel A) and market share (panel B) by product type across 97 countries.
Conventional tobacco products include various forms of smoked tobacco such as manufactured cigarettes, roll-your-own tobacco, shisha, bidis and kreteks. Smoking remains the primary delivery mechanism for tobacco globally, with 80% of all tobacco users smoking — 16.7% of all people aged 15 years and older are current tobacco smokers. Cigarettes predominate, with 89% of those smoking tobacco smoking cigarettes (15.0% of all people aged ≥15 years).
Smokeless tobacco products include chewing tobacco and newer tobacco products such as snus. Although less prevalent globally, these products constitute a major proportion of tobacco use in some regions — most notably the WHO South-East Asia Region, where 18% of adults use smokeless tobacco, and the WHO Eastern Mediterranean Region, where 5% do.
The main commercial and non-therapeutic nicotine products are ENDS and nicotine pouches. Understanding the prevalence of ENDS use is important, as these are health-harming and addictive products and studies show that young people who use e-cigarettes are almost three times more likely to use cigarettes later in life. In some countries the rates of e-cigarette use among young people have surpassed those of adults: in Canada in 2019, e-cigarette use within the last 30 days at time of survey among schoolchildren in grades 7–9 (typically 12–15 years) was 11%, whereas among Canadian adults it was less than 5%; in France in 2021, 14% of children in 9th grade (typically 14–15 years) were current users of e-cigarettes, whereas less than 7% of adults were.
Panel 1: New and emerging products
According to WHO, new and emerging tobacco and nicotine products must meet at least one of the following criteria:
- New or unconventional technology is used, such as vaporisation of tobacco into the lungs or use of menthol pellets in a cigarette filter.
- The product type has been on the market for less than 12 years; these products include dissolvable tobacco products.
- The product type has been on the market for longer than 12 years, but the market share has increased in areas in which this type of product was not traditionally used (such as smokeless tobacco products being introduced into countries where they were not previously available).
- The product is marketed with the claim that it could reduce exposure to harmful chemicals.
Burden of disease
The global burden of disease and mortality attributable to tobacco use is substantial. In 2023, tobacco resulted in 7.4 million deaths (95% CI 6.4–8.5) and 204 million disability-adjusted life-years (DALYs; 171–236).1 Although second-hand smoke exposure results in fewer deaths than tobacco use, more than 64% of second-hand-smoke-related deaths occur among women.
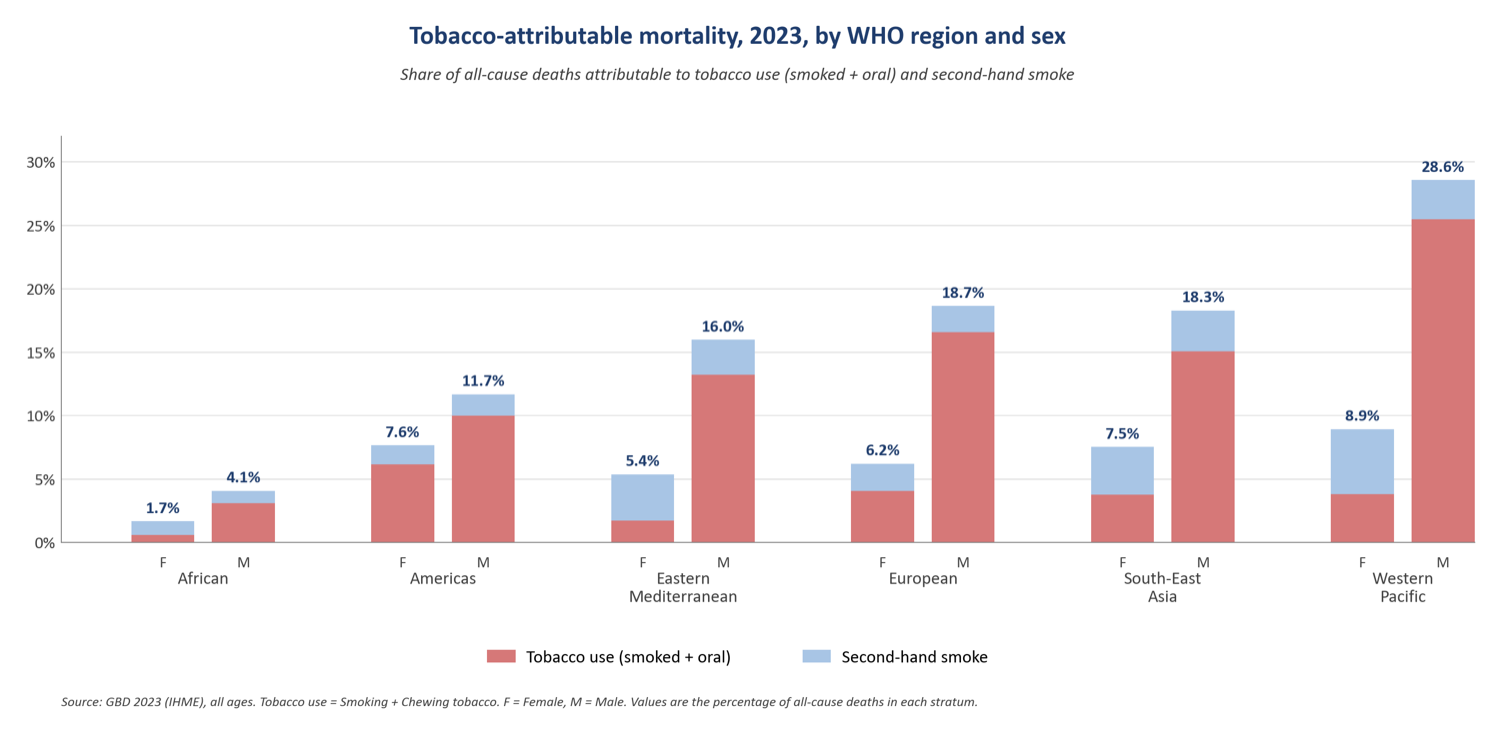
Figure 5 (updated with Global Burden of Disease 2023 data): tobacco-attributable mortality by WHO region and sex, as a share of all-cause deaths (tobacco use plus second-hand smoke).
The burden of smoking-attributable mortality varies across populations, countries, regions and over time. In 1990, more than 20% of deaths in men older than 30 years in several countries — including the USA, Canada, much of Europe, Australia, New Zealand, Japan, southern Latin America, China, Malaysia and the Philippines — were attributable to smoking. By 2020, although the fraction of deaths due to smoking had declined in many high-income countries, this proportion remained greater than 20% in eastern and central Europe, Spain, Egypt, the Philippines, China and Indonesia.
Respiratory diseases are a major consequence of tobacco use. Approximately 30% of deaths and DALYs from chronic obstructive pulmonary disease (COPD) and about half of the deaths and DALYs from lung cancer are attributable to smoking, making it the leading cause of these major respiratory conditions. In many countries, lung cancer rates among women are beginning to exceed breast cancer mortality rates, reflecting the delayed effect of increasing smoking prevalence.
The implications of new and emerging tobacco and nicotine products on the burden of disease are not yet fully understood. Although often marketed as less harmful alternatives to tobacco, they pose several risks to health and the full scope of their long-term health effects remains uncertain. ENDS devices have been established to generate toxic substances, some of which are known to cause cancer and increase the risk of heart and lung disorders. Their use is likely to be associated with asthma and COPD, and can affect brain development leading to serious consequences like learning and anxiety disorders. Exposure to their emissions among pregnant people can similarly affect fetal brain development. Moreover, exposure to their emissions might pose risks to bystanders. It is important to note that ENDS are often used as complements to, and not substitutes for, conventional cigarettes — and this dual use seems to be linked with increased risk of cardiovascular and respiratory conditions compared with the single use of one of these products.
Tobacco control policies
The WHO FCTC has been the foundation of global tobacco control efforts since 2005. An impact assessment after 12 years of implementation showed substantial gains, but also great variability across countries and policy areas — higher WHO FCTC implementation levels were correlated with greater reductions in smoking prevalence.
A recent analysis by Paraje and colleagues of the effect of the first 10 years of the WHO FCTC after ratification shows substantial positive effects. The treaty has led to a decrease in the prevalence of smoking in people younger than 25 years, with 24 million fewer people younger than 25 smoking. An increase in the quitting ratio — with 2 million more people aged 45–59 quitting — has also been observed. Specifically, the quitting ratio at baseline was 0.34; after WHO FCTC ratification, this increased by an annual average of 0.1% for a total cumulative increase of 1.8% compared with pre-ratification trends. At least 12 million deaths are estimated to have been averted by just one decade of the WHO FCTC’s implementation. Countries that increased tobacco taxes by more than 10% after ratification achieved substantially better results in decreases in smoking prevalence and quit ratios than those that did not. This analysis contradicts an earlier 2019 study by Hoffman and colleagues which found no significant effect — the Paraje study stands out for its more recent data, broader range of indicators, far larger country sample (171 versus 71), focus on specific age groups, consideration of implementation factors such as taxation, and ample set of alternative statistical models.
The implementation of the MPOWER technical package has helped to reduce the prevalence of tobacco smoking. Without these declines, there would be 300 million more smokers today.
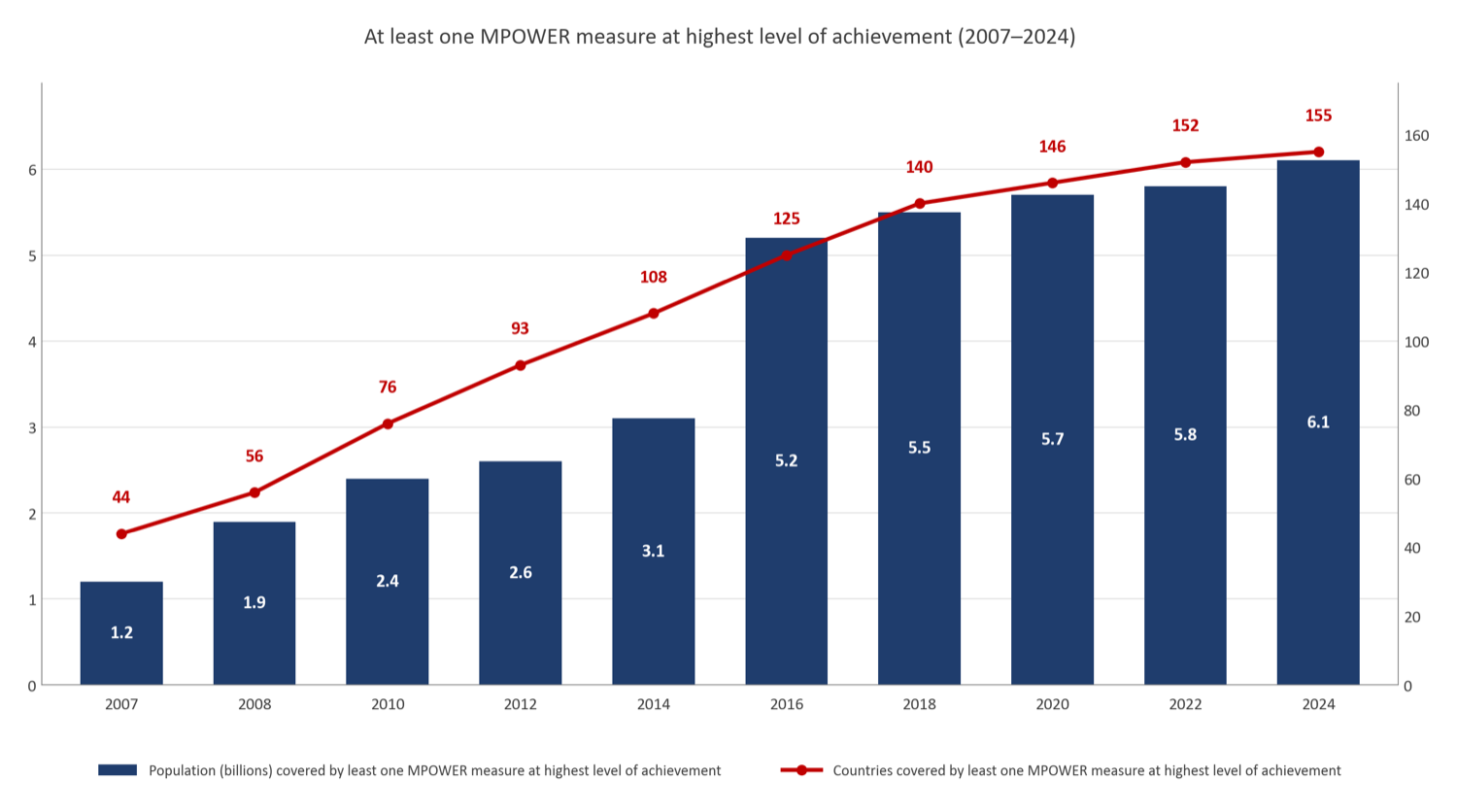
Figure 6 (redrawn): population and number of countries covered by at least one measure at the highest level of achievement from the MPOWER technical package, 2007–2024.
Gravely and colleagues found that each additional measure implemented at the highest level between 2007 and 2014 was associated with an average decrease in smoking prevalence of 1.57% between 2005 and 2015 — a relative decrease of 7.09%. In addition, there is evidence to suggest that the effect of the WHO FCTC in general and of MPOWER in particular might be underestimated in some studies due to the non-inclusion of some benefits: many analyses do not account for the denormalisation of tobacco use or the reduction in exposure to second-hand smoke, which have major health benefits (particularly for non-smoking adults and children). Similarly, Levy and colleagues noted that the effect of newly implemented policies could extend beyond reductions in smoking-attributable deaths to include benefits in other smoking-related outcomes, such as reduced adverse birth outcomes related to maternal smoking, better quality of life, lower health-care costs, and less productivity loss.
Tobacco taxes
Raising taxes on tobacco products has been identified as the most effective individual tobacco control measure. Goodchild and colleagues estimated that increasing excise tax by $1.00 per 20 cigarettes would increase the mean retail price of cigarettes by 42%, reduce global cigarette consumption by 18%, and increase cigarette excise revenue by $190 billion worldwide. The additional excise revenue could help create the fiscal space needed by countries to meet their development priorities, potentially increasing public expenditure on health by 4% globally. The prevalence of daily cigarette smoking among adults would decline by 9%, translating into 66 million fewer smokers and a decrease of 15 million smoking-attributable deaths. Despite the measure’s potential for unlocking immediate and medium-term revenue gains and its enormous cost-effectiveness as a health intervention, tobacco taxes are one of the measures least implemented at a best-practice level — only 1.2 billion people are living in countries with best-practice levels of implementation.
Smoke-free legislation
Implementation of comprehensive smoke-free laws has been associated with substantial health benefits. Akter and colleagues found that smoke-free legislation was associated with a 9–10% reduction in overall cardiovascular disease events (acute myocardial infarction, coronary heart disease, cerebrovascular disease and sudden cardiac death), a 9% reduction in cardiovascular disease–related hospitalisations, and a 16–17% reduction in respiratory disease mortality. At present, a total of 2.6 billion people are protected with best-practice smoke-free laws.
Health warnings
Graphic health warnings on tobacco products have been found to increase the knowledge among people who smoke of risks and to lead to increases in the intention to quit. They have been widely implemented, with 110 countries adopting such policies at the level of best practice, protecting more than 5.1 billion people. Many countries are going beyond health warnings to implement plain packaging — which not only diminishes the appeal of packaging but also enhances the effect of the graphic health warnings. This policy is particularly important for decreasing tobacco use uptake among children, who are more responsive to packaging signals.
Advertising bans
Tobacco advertising, promotion and sponsorship (TAPS) plays a key role in young people’s initiation of tobacco use and in maintaining and increasing tobacco use among new and existing users. TAPS bans are associated with a 20% reduction in the odds of current smoking and a 37% reduction in the risk of smoking initiation. In 2024, of the 68 countries with comprehensive TAPS bans covering just over 2 billion people, 12 were low-income, 38 were middle-income and 18 were high-income. Although almost half of all low-income countries have a best-practice TAPS ban in place, only one-third of middle-income countries and one-quarter of high-income countries have achieved this. Despite its effectiveness, this is among the most under-adopted measures of the WHO FCTC.
Cessation support
Tobacco cessation improves quality of life and reduces the risk of premature death — smoking cessation can add about a decade to life expectancy and, although the benefits are greater when younger, cessation at any age will improve health. Quitting smoking decreases the risk of lung cancer and of developing COPD. Cessation services, including both pharmaceutical and behavioural interventions, have been shown to support quitting. Although fewer countries have implemented comprehensive cessation services, those that have done so cover almost 2.7 billion people.
Collective use of control measures
These five measures have collectively had a substantial effect. Ngo and colleagues found that a one-unit increase in the MPOWER composite score was associated with a reduction of 0.2% in adult smoking prevalence and 0.3% in smoking prevalence among men. These effects are even more impressive when considered cumulatively: if a country implemented all MPOWER measures at best-practice levels, this would mean a 7.26% reduction in adult smoking prevalence.
These evidence-based and cost-effective measures are more effective when implemented as part of a package because they are mutually reinforcing. Based on WHO analysis, raising tobacco taxes and implementing comprehensive smoke-free laws are the two most effective and cost-effective measures within MPOWER and should be a priority for all countries. At the same time, all these interventions are highly impactful and cost-effective, which means prioritisation at national level might need to account for other factors such as implementation and enforcement capacity, the existing regulatory powers available to the health sector, and the political opportunities available for fiscal and legislative reform.
WHO-CHOICE economic analyses for MPOWER measures
Health effect measured in healthy life-years gained, per million people per year.
| Measure | Low-income (years gained) | Lower middle-income (years gained) | Upper middle-income (years gained) |
|---|---|---|---|
| Raising taxes on tobacco products | 1717 | 2674 | 3093 |
| Health warnings and standardised / plain packaging | 1212 | 2181 | 2319 |
| TAPS bans | 933 | 1490 | 1535 |
| Comprehensive smoke-free laws | 1475 | 2845 | 3077 |
| Mass media campaigns | 1345 | 2516 | 2701 |
| Cessation support | 1028 | 1724 | 1800 |
Economic cost for each is under I$ 0.10 million (international dollars) per million people per year across all income groups — consistently among the most cost-effective public health measures available.
The foundation for achievement and progress on these and all measures under the WHO FCTC is Article 5.3, which calls for the protection of public health policies with respect to tobacco control from commercial and other vested interests of the tobacco industry. In 2023, 72% of WHO FCTC Parties reported the adoption or implementation of at least one measure recommended in the guidelines for implementation of Article 5.3. Much more needs to be done, since industry interference is one of the main obstacles to the implementation of the WHO FCTC in the majority of countries. Article 5.3 and all the WHO FCTC’s measures are also needed and effective in responding to new and emerging nicotine and tobacco products.
Panel 2: Responding to new and emerging nicotine and tobacco products
The introduction, increasing uptake and aggressive marketing — particularly to young people and with misleading or fake health claims — of new and emerging tobacco and nicotine products is another major challenge. The response should be focused on the regulation of these products, which is in general insufficient, with many countries having no regulations. As tobacco products, HTPs are subject to the provisions of the WHO FCTC and, where they are not banned, need to be given equivalent regulatory and fiscal treatment as other tobacco products. Similarly, where not banned, ENDS can be addressed with demand-reduction measures and, in particular, a focus on regulating marketing and product design to prevent unproven health claims and efforts to promote these products to young people. The challenge posed by the political and public relations machine behind ENDS and HTPs is focused on interfering in policymaking and science, gaining access to decision-making, and ultimately weaponising these products within a redemption narrative that aims at splintering global tobacco control. As a response, Article 5.3 needs to be applied across the board for all businesses, organisations and individuals involved in or affiliated with the tobacco and nicotine industry.
Challenges
The overarching challenge in tobacco control is the fact that, despite progress in the implementation of the WHO FCTC, the introduction of different measures has been uneven across countries and policy domains. In general, the overall implementation level has also been insufficient, considering that the WHO FCTC has been in force for almost 20 years. In addition, as of 2025, 12 WHO Member States encompassing about 750 million people are not yet Parties to the WHO FCTC. The consequences can be seen in the fact that, as of 2024, 40 countries had not yet adopted any single demand-reduction measure from the WHO MPOWER technical package at best-practice level, leaving almost 2 billion people vulnerable to the harms of tobacco. The pace of implementation has also slowed since 2018 — particularly for tobacco taxation, for which implementation has progressed the least.
In the last session of the Conference of the Parties, the Expert Group on Forward-Looking Tobacco Control Measures was created with the mandate of identifying and describing forward-looking measures and measures that expand or intensify approaches to tobacco control. The foundation for this decision was the uneven progress in implementation, the fact that some Parties have been advancing forward-looking tobacco control measures, together with the changing landscape of the tobacco epidemic and the ever-evolving tactics of the tobacco industry.
Panel 3: Implementing forward-looking tobacco control measures
For some jurisdictions concerns might exist that the tobacco industry’s business model and its continued capacity to exercise power over politics and science, along with its ability to adapt and refine interference strategies, make its continued operation as a commercial enterprise an untenable barrier to progress in tobacco control. A case can be made in favour of sunsetting commercial tobacco products or the entire commercial tobacco industry as part of a way of addressing the root cause of the epidemic. However, this question has not been addressed by Parties to the WHO FCTC and remains subject to further consideration. There is also value in maintaining focus on determined efforts at accelerating progress on the path already set out by the demonstrated success of many countries in reducing tobacco use through high levels of WHO FCTC implementation. This focus is crucial because end-game policies — in which the goal is to entirely or near-entirely eliminate tobacco use — are likely most feasible in countries with both low smoking prevalence and high levels of WHO FCTC implementation.
Insufficient funding and enforcement
One of the two main implementation barriers identified by WHO FCTC Parties is insufficient funding. This creates multiple constraints: little political attention, inadequate monitoring and surveillance capacities, weak enforcement of existing measures, and reduced efforts towards more ambitious measures. Although related to resourcing, enforcement of both existing and new tobacco control measures is a major issue in many countries even where resources are available. Progress in getting laws, regulations and fiscal measures through parliaments and policymaking processes will not reduce tobacco use or improve health without concerted and sustained effort in enforcement — which often requires more political will and is more costly and complicated than passing or adopting the underlying instruments. Part of the solution is prioritisation: it is important for Parties to focus on the most cost-effective measures, such as protecting people from exposure to tobacco smoke (Article 8) or graphic health warnings on tobacco packages (Article 11). After almost 20 years of being in force, these measures should be quasi-universal, since they are also part of the comprehensive mandates of ministries of health. Finally, to be able to continue monitoring the evolution of the epidemic, it is key for countries to invest in epidemiological surveillance — especially for monitoring of smoking prevalence, tobacco consumption and mortality data.
Industry interference
The other main implementation barrier identified by WHO FCTC Parties is the interference of the tobacco industry. The tobacco industry will never stop its efforts to undermine tobacco control until it ceases to operate as an industry. The common practices of the tobacco industry can be countered by identifying them and applying the guidelines to Article 5.3. These practices include:
- Political practices — lobbying of lawmakers to block or weaken legislation; suing governments to delay or overturn laws.
- Scientific practices — spreading false information about health risks or about doomsday consequences from the implementation of tobacco control policies; creating biased scientific evidence that downplays the health or economic effects of tobacco.
- Image laundering — funding of social programmes to falsify the industry’s public image.
To address the industry interference challenge, it is imperative to strengthen the implementation of Article 5.3 and its guidelines, including: minimising interactions and ensuring transparency when dealing with the tobacco industry; avoiding conflicts of interest and rejecting non-binding agreements; raising awareness about tobacco industry tactics to undermine public health policies; and denormalising corporate social responsibility activities by the tobacco industry.
Tobacco industry’s interference exploits prevailing political economies in ways that can impede progress on tobacco control. This issue is particularly prevalent in countries with politically salient tobacco growing and manufacturing operations. It is important to counter the tobacco industry’s economic arguments by drawing on extensive existing evidence that tobacco causes far greater economic harm than benefit and that other sectors can provide equivalent economic value without the associated costs. One promising solution for countries with tobacco farming is implementation of WHO FCTC Article 17 programmes for alternative livelihoods, such as the UN Tobacco-Free Farms Initiatives, which promote economically viable alternatives by identifying equivalent or more advantageous crops and providing the financing, market access and marketability guarantees that can facilitate the agricultural transition. In the case of taxes, it is important to increase the synergy with ministries of finance and other financial institutions to counteract the SCARE tactics used by the tobacco industry to discourage governments considering tobacco tax increases.
Beyond these across-the-board challenges for tobacco control, there are several specific challenges, responses needed and opportunities available in respiratory diseases. This disease-specific focus is required because the complex interplay between tobacco use, other exposure-based risk factors and communicable disease is important for lung health, treatment and management across the life-course. These factors interact synergistically, exacerbating lung infections and chronic respiratory diseases.
Related to these specific challenges for lung health is the first ever WHO Director-General Special Envoy for Chronic Respiratory Diseases, established in June 2024. This new development presents an opportunity to bring together a primary health-care approach, community and partner mobilisation, as well as new approaches to the commercial determinants of health — a framework for understanding and addressing business effects on health and health equity. The Envoy will be focused on raising awareness, mobilising support and implementing effective solutions to improve respiratory health worldwide — elevating the profile of tobacco control within the broader respiratory health agenda and respiratory health within the tobacco control agenda.
Conclusions and recommendations
Addressing the challenges in tobacco control requires a multifaceted approach that combines strong policy implementation, enhanced global cooperation, and tailored interventions for specific demographic groups. By strengthening the implementation of the WHO FCTC, countering industry interference, regulating new products, and addressing the needs of diverse populations, countries can progress in reducing the global burden of tobacco use. But this effort requires sustained political will, adequate resources and ongoing adaptation to the evolving tobacco landscape.
Specific recommendations include:
- Strengthening and accelerating the implementation and enforcement of the WHO FCTC, with focus on the most cost-effective measures (i.e. tax increases, smoke-free environments, and big graphic health warnings on tobacco packages).
- Countering the interference of the tobacco industry in public health and science by scaling up implementation of the guidelines for implementation of Article 5.3.
- Increasing domestic investment in tobacco control measures that have shown a high return on investment.
- Strengthening epidemiological surveillance — especially for smoking prevalence, consumption and mortality data.
- Increasing research on the health consequences of new tobacco and nicotine products, particularly on their long-term effects.
Footnotes
-
These global burden figures have been updated from the Global Burden of Disease 2021 estimates cited in the published paper to the latest GBD 2023 estimates (IHME); the regional breakdown in figure 5 is updated on the same basis. ↩