Types, Costs, Benefits and Resourcing of Community-led and Other Responses for SRHR: A Scoping Review

Written by Juliette McHardy, Maïmouna Bah and Agrata Sharma with data visualisations and analysis by Quincy Jones. Produced by the HIV Policy Lab team of the Global Health Policy and Politics Initiative at the O’Neill Institute for National and Global Law. Washington, D.C., October 2022.
The review was developed through an extended programme of consultation with Love Alliance partners, bilateral partners and civil society.
Abstract
Introduction
This scoping review’s overarching objective is to promote investment in and reliance on community-led responses for the sexual and reproductive health rights of HIV’s key and vulnerable populations. It does this by mapping evidence on the financial resource requirements and benefits of these responses as well as the costs of inaction on the law and policy determinants of sexual and reproductive health and rights. While there are previous and forthcoming evidence syntheses on community responses and on the law and policy determinants, no studies seek to bring these siloed bodies of evidence into dialogue with one another and, thereby, interrogate the interdependency of community empowerment and legal environments for enabling sexual and reproductive health.
Methods and analysis
The scoping review was conducted in accordance with the JBI Manual for Evidence Synthesis methodology and has been registered with the Open Science Framework. MEDLINE, Embase, Web of Science, Sociology Abstracts, EconLit and Google Scholar were searched. All sources were screened for relevance, assessed for inclusion and subjected to data extraction by two independent researchers, with a third researcher intervening in case of disagreement.
Sources concerned with HIV and the responses of key and vulnerable populations were eligible for inclusion when they explored community-led responses for sexual and reproductive health rights or the law and policy determinants of sexual and reproductive health. These sources also had to explore the costs, benefits or financial resource requirements of these interventions.
Results
A large proportion of sources on community-leadership touch on its potential for improving legal determinants. The sources also show how the legal environment can be both a barrier to and an enabler of community leadership. Taken together, these cross-cutting sources indicate a literature that explores, albeit infrequently overtly, the mutuality of community leadership and legal determinants.
The types of community-led responses described in the literature vary significantly in terms of the community ownership over these responses, and the degree of community ownership appears to affect the priorities and aims of these responses. As community ownership increases, the types of community-led responses seen become more diverse and less narrowly focused on service delivery. The included sources substantiate the already well-evidenced benefits of community-led responses but also show that few sources describe these benefits in terms of cost-effectiveness.
There are few studies providing precise measures of the financial resource requirements. There is often a reliance on underpaid or unpaid labour from volunteers within the community. A large number of the sources describe resource requirements in terms of the challenges of unreliable, insufficient or overly prescriptive funding.
The sources more commonly feature laws, policies and practices that negatively impact sexual and reproductive health and rights. The most common pathway for negative impact is discrimination and criminalisation, and the most common pathway for positive impact is anti-discrimination and decriminalisation. Negative laws, policies and practices are characterised in the literature as undermining access, availability and quality of health services and also undermine health-promoting behaviours, with various direct harms to health consequent to this. Positive laws, policies and practices vary but highlight in particular the limitations of isolated reforms and the need for concerted approaches of mutually-supportive legal reforms as well as broader societal interventions.
Conclusions
This review demonstrates how fundamental attention to the legal determinants is for realising the full potential of community-led responses and ensuring progress on ending HIV and preventing deaths from AIDS. It also confirms the interrelationship between investment in community leadership and realisation of progress on the societal enablers. The included sources also show that community-led responses are of significance in improving the legal determinants, and such improvements are a common aim and outcome of community-led responses.
This review supports investment in and advocacy for community-led responses to HIV and related sexual and reproductive health challenges. All sources cite benefits to health, and community-led responses are shown to have impact in delivering health services, ensuring prevention and moving the needle on critical legal determinants and related societal enablers. At the same time, funding challenges make delivering the services or programming needed challenging, difficult or impossible. More subtly, they can also warp the character of the community-led response by requiring communities to fit the prescriptions and reporting requirements of funders rather than the needs and processes preferred and most suited to the communities themselves. High-quality and high-ownership community-led responses require capacitation and organisational development over the long-term, which makes sustained and predictable funding essential.
The literature is disproportionately focused on limited, time-bound and low-community-ownership responses that do not and cannot capture the benefits and value of community leadership. There is insufficient research on the financial and other resource requirements of community-led responses, as well as on the overall share and character of community-led responses within the HIV response. There is also a need for further research on how positive legal determinants enable and strengthen community-led responses and how negative legal determinants undermine and frustrate them.
Scoping review purposes
Sexual and reproductive health services and rights are systematically denied communities and people on the basis of their actual or perceived health status, sexual orientation, gender identity, sex characteristics and behaviours. Those belonging to one or more of these vulnerable and marginalised communities are less likely to enjoy sexual and reproductive health and more likely to suffer from reduced access to high-quality sexual and reproductive health services. This is a function of negative legal determinants of health — including actively discriminatory and criminalising laws, policies and practices, as well as the absence of laws and policies for protecting and fulfilling sexual and reproductive rights by eliminating discrimination and providing for substantive equality in health services. Responses led by affected communities are effective at ensuring access to quality health services and improvements in the legal determinants but are underfunded, underutilised, and often stunted by inhospitable or even punitive legal environments that deny them their rights and ability to organise.
With or without official recognition, communities have often led their own responses to counter neglect, discrimination and criminalisation — with mutual aid strategies of community prevention, treatment and care in substitution for denied or inadequate health-sector-provided services, as well as through advocacy and organised resistance against the laws, policies and practices that abridge their sexual and reproductive rights. Community-led organisations will better improve health outcomes and the legal environment when sustainably financed, integrated as a complement to the health sector, accorded legal recognition, protected from discrimination, and able to cooperate with public actors responsible for key upstream determinants of health.
In response to the immense success and proven potential of community-led responses, the Love Alliance commissioned this review. The Alliance is a consortium of community-led organisations operating across Burkina Faso, Burundi, Egypt, Kenya, Morocco, Mozambique, Nigeria, South Africa, Uganda and Zimbabwe, in partnership with Aidsfonds and the Global Network of People Living with HIV (GNP+). This review adopted the definition of community-led responses arrived at in a June 2019 consultation convened by UNAIDS: community-led responses comprise a diverse set of interventions carried out at varying scales and levels, but are all informed, implemented and determined by communities for their own members.
A model for progress exists in the Global AIDS Strategy 2021–2026, which links the 30-80-60 targets on community-led responses with the 10-10-10 targets for improvements in the societal enablers of the HIV response, which, in turn, need to be underpinned by action on the legal determinants. The Strategy’s model contains the potential for catalysing progress on sexual and reproductive health challenges — firstly through its prioritisation of community-led delivery of health services and programmes supportive of the legal and social determinants, and secondly by creating space for genuinely community-led responses that is, itself, reliant on improvements in the laws, policies and practices that drive progress on the societal enabler targets. Implementation is, however, preconditioned on intergovernmental actors, national governments and other funders addressing their deficit of political will and closing financing gaps. This review intends to narrow the gap between aspiration and achievement.
Review questions
- With a focus on HIV and related health challenges experienced by key and vulnerable populations, what are the types, costs, benefits and financial resource needs for community-led delivery of sexual and reproductive health services and responses to stigma, discrimination, criminalisation and gender inequality?
- With a focus on HIV and related sexual and reproductive challenges, what are the costs of implementing discriminatory and criminalising laws, policies and practices targeting marginalised communities and key populations and, conversely, what are the benefits of implementing non-discriminatory and rights-affirming laws and policies?
Search strategy and methods
The review was developed using a participatory action research strategy grounded in the guidance of Fran Baum and collaborators and Laurel Sprague and collaborators, and followed JBI Manual methodology for scoping reviews. It was registered with the Open Science Framework, with the search strategy informed by the PRESS Peer Review Guideline Statement and the de-duplication methods of Bramer and collaborators. Eligibility criteria were structured using the JBI participant-concept-context framework, and reporting follows PRISMA-ScR.
Databases searched included MEDLINE and Embase (via Ovid), Web of Science (via Clarivate), Sociology Abstracts (via ProQuest), EconLit (via EBSCO), and — for grey literature — Google Scholar and ProQuest Dissertations and Theses, supplemented by targeted searches of specific sexual and reproductive health journals. Expert consultation extended across UNAIDS, UNDP, the Global Fund, the Gates Foundation, the World Bank, WHO, the Johns Hopkins Bloomberg School of Public Health, the Geneva Graduate Institute, the Drexel Dornsife School of Public Health, and the USC Institute on Inequalities in Global Health, and meaningful consultation with Love Alliance partners was conducted across two sets of partner meetings. In response to partner feedback on preliminary results, a variable grading Aim 1 sources by their degree of community ownership was introduced and subsequently refined.
Participants targeted were the HIV responses of key populations (people living with HIV, men who have sex with men, transgender people, people who inject drugs, and sex workers and their clients) and vulnerable populations (at minimum, women and girls — in particular adolescent girls and young women — as well as incarcerated people and others living in closed settings). Concept included community-led responses for guaranteeing sexual and reproductive health services and rights related to HIV or improving the societal enablers (Aim 1), and the legal determinants of the HIV response with a focus on rights-affirming and non-discriminatory as well as criminalising, discriminatory and stigmatising measures (Aim 2). To be community-led, responses had to centre community leadership in a way that goes beyond tokenism, mere engagement or circumscribed co-creation.
All identified citations were de-duplicated in EndNote 20, screened in Rayyan, and assessed for inclusion in Covidence, with disagreements resolved by a third reviewer. Data was extracted using a modified Covidence tool piloted and revised during extraction. Results are presented graphically and with tables accompanied by a narrative summary describing how they relate to each aim.
Results
Our search strategy identified 6,093 sources, of which 3,291 were unique and 2,802 duplicates. After title/abstract screening, 958 sources plus a further 194 handpicked sources (from pre-scoping searches, expert consultation and bibliographies of key sources) were subjected to full-text eligibility assessment — 1,143 sources in total. Of these, 356 were included, with 86 coded as relevant to Aim 1, 253 as relevant to Aim 2, and 16 as relevant to both aims.
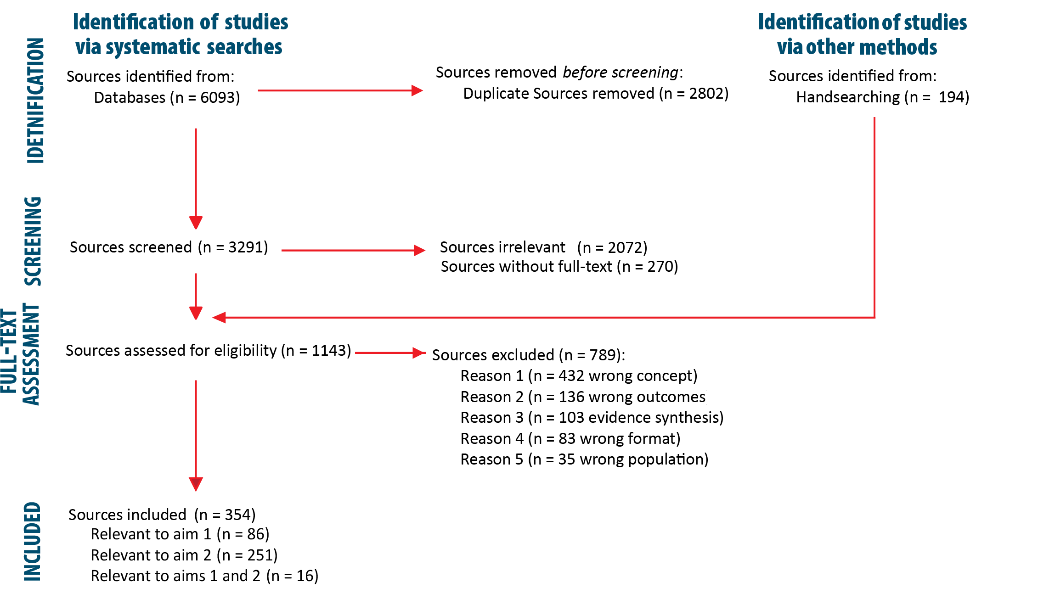 Figure 1 — PRISMA-ScR flow diagram of identification, screening and inclusion.
Figure 1 — PRISMA-ScR flow diagram of identification, screening and inclusion.
Aim 1: community-led responses
Trends. The majority of included sources were published within the last four years, with a steady upward trend reflecting both substantive shifts in the types of community responses being actioned, funded and documented (e.g. the Global Fund’s 2010 Community Systems Strengthening Framework and the 2016 Political Declaration on HIV and AIDS) and shifts in the terms and language used to describe community-led responses.
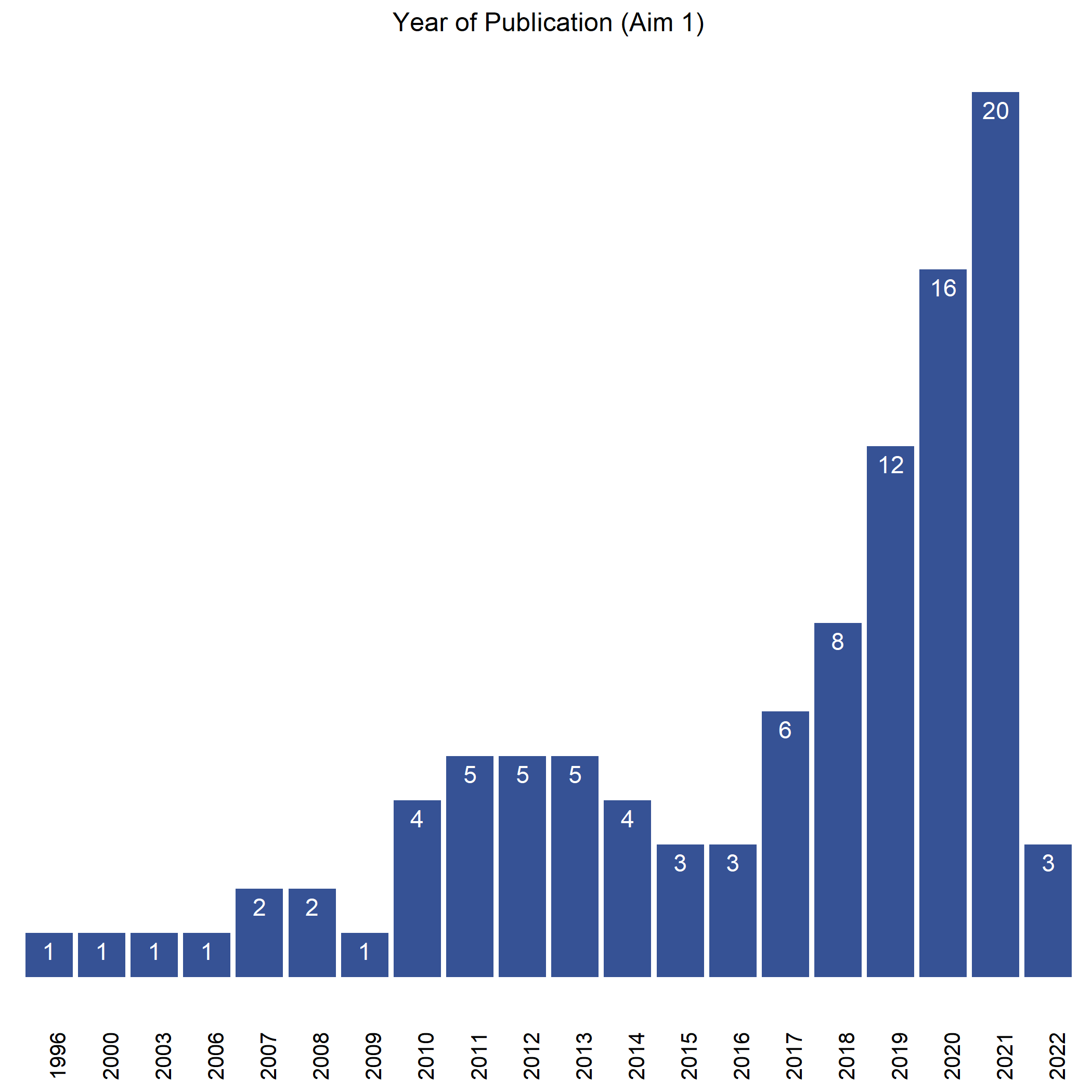 Figure 2 — Aim 1 sources by year of publication.
Figure 2 — Aim 1 sources by year of publication.
Settings. Of 103 Aim 1 sources, 21 explore a Love Alliance partnership country setting; Morocco and Egypt do not feature, likely owing to the English-language limitation. A further 56 sources explore comparable settings (neighbouring regions or other low- and middle-income countries), while 26 focus on high-income settings coded as dissimilar. Two constellations of organisations and responses dominate the literature: those associated with the Gates-funded Avahan India AIDS Initiative (22 sources, including Project Parivartan, Project Pragati, Swasti, Care-Saksham, Swathi Mahila Sangha, Nari-Saksham and — most notably — the Ashodaya Samithi collective, the focus of nine sources) and those associated with the Durbar Mahila Samanwaya Committee (DMSC) and its associated organisations SANGRAM and the VAMPs collectives (four sources).
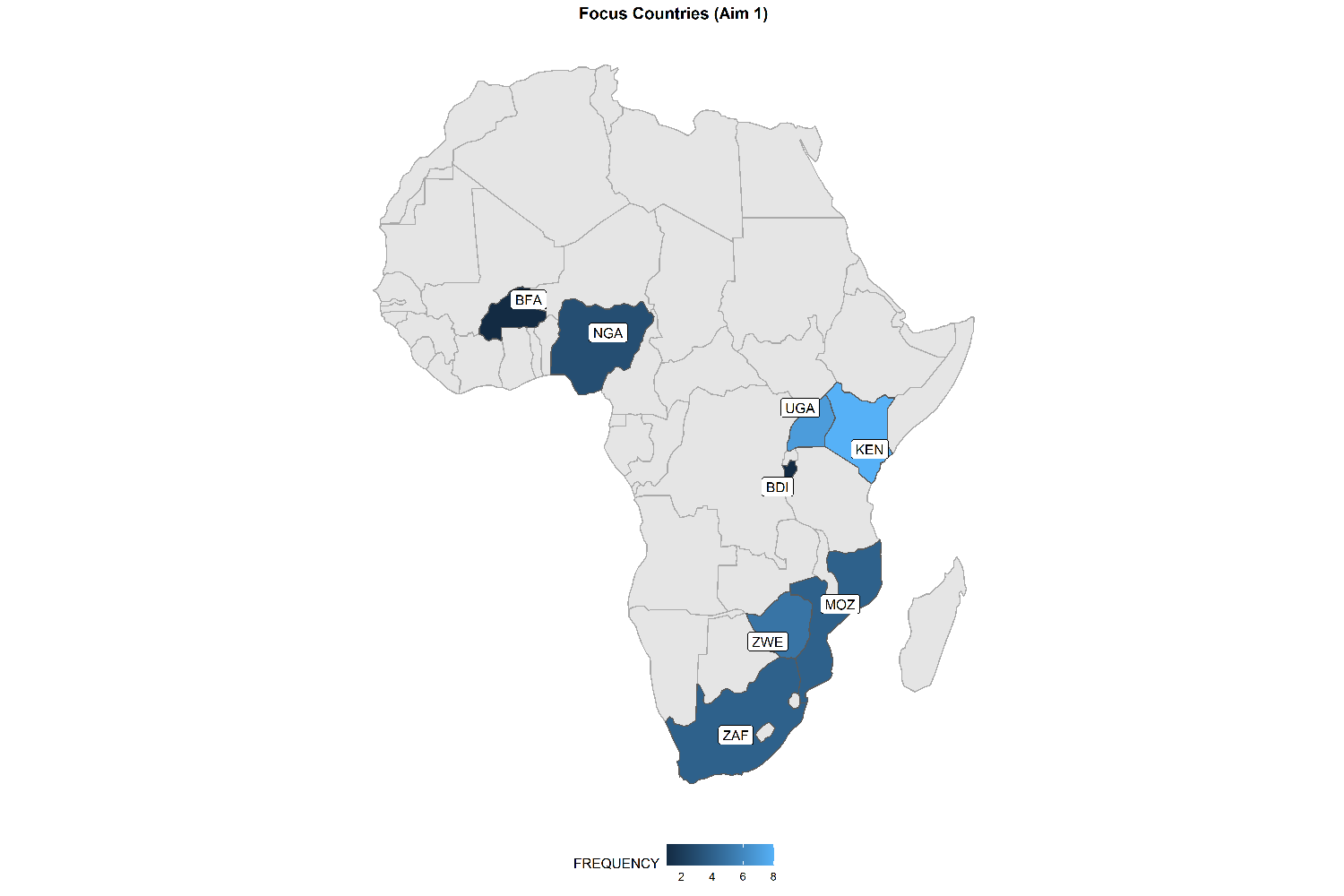 Figure 3 — Focus countries of Aim 1 sources.
Figure 3 — Focus countries of Aim 1 sources.
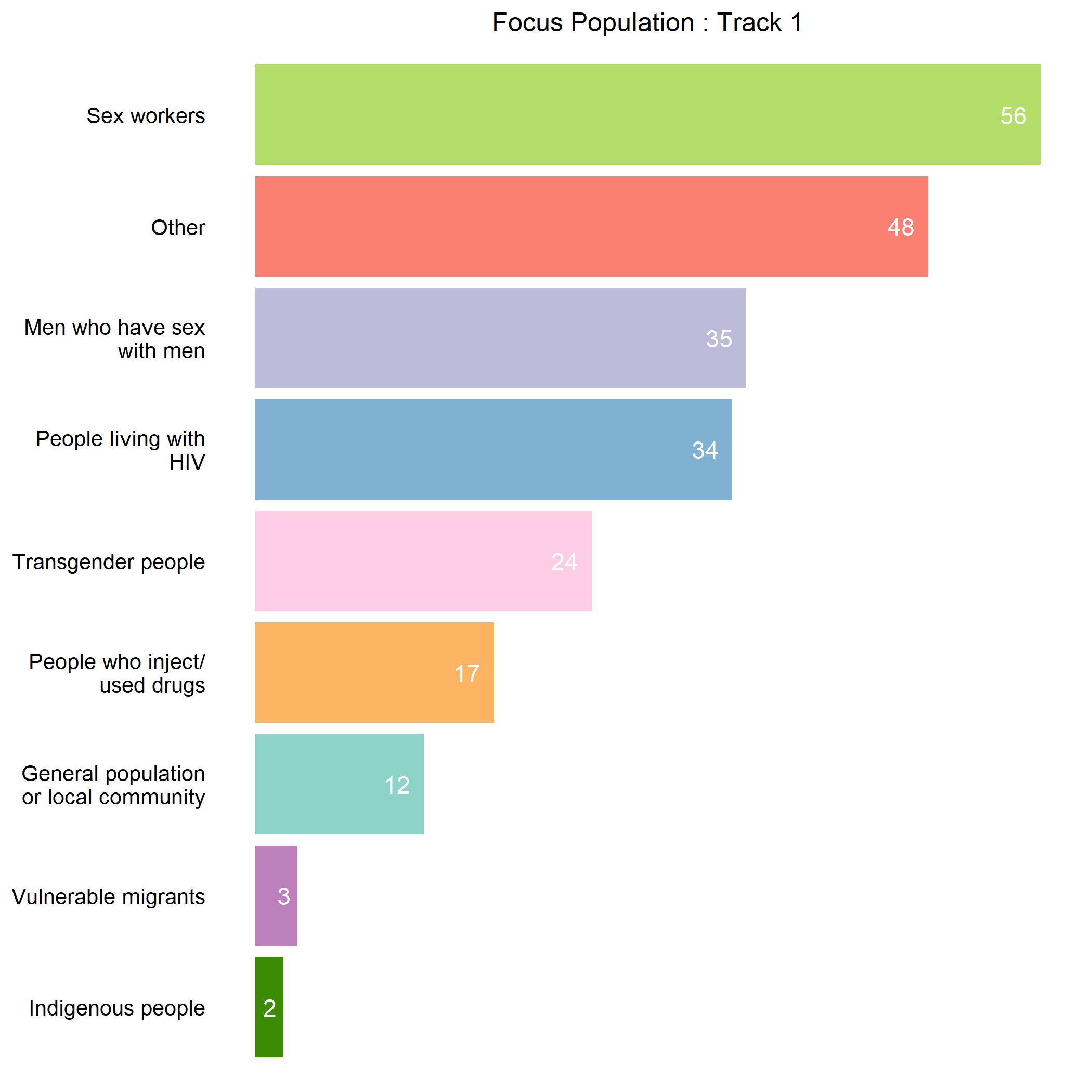 Figure 4 — Populations featured across Aim 1 sources.
Figure 4 — Populations featured across Aim 1 sources.
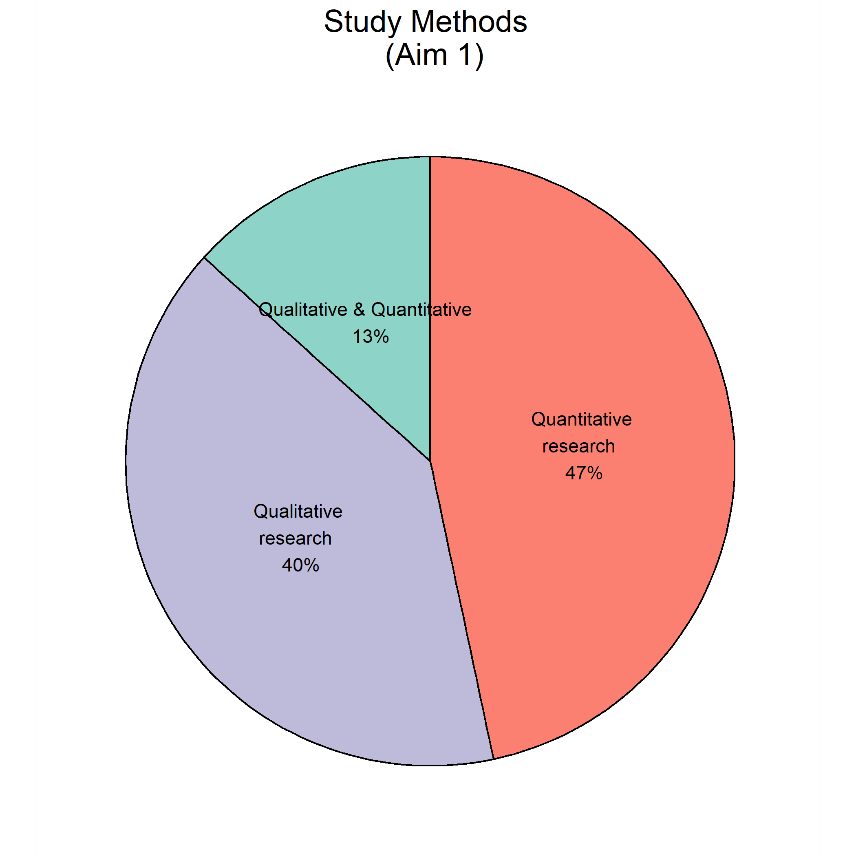 Figure 5 — Study methods used across Aim 1 sources.
Figure 5 — Study methods used across Aim 1 sources.
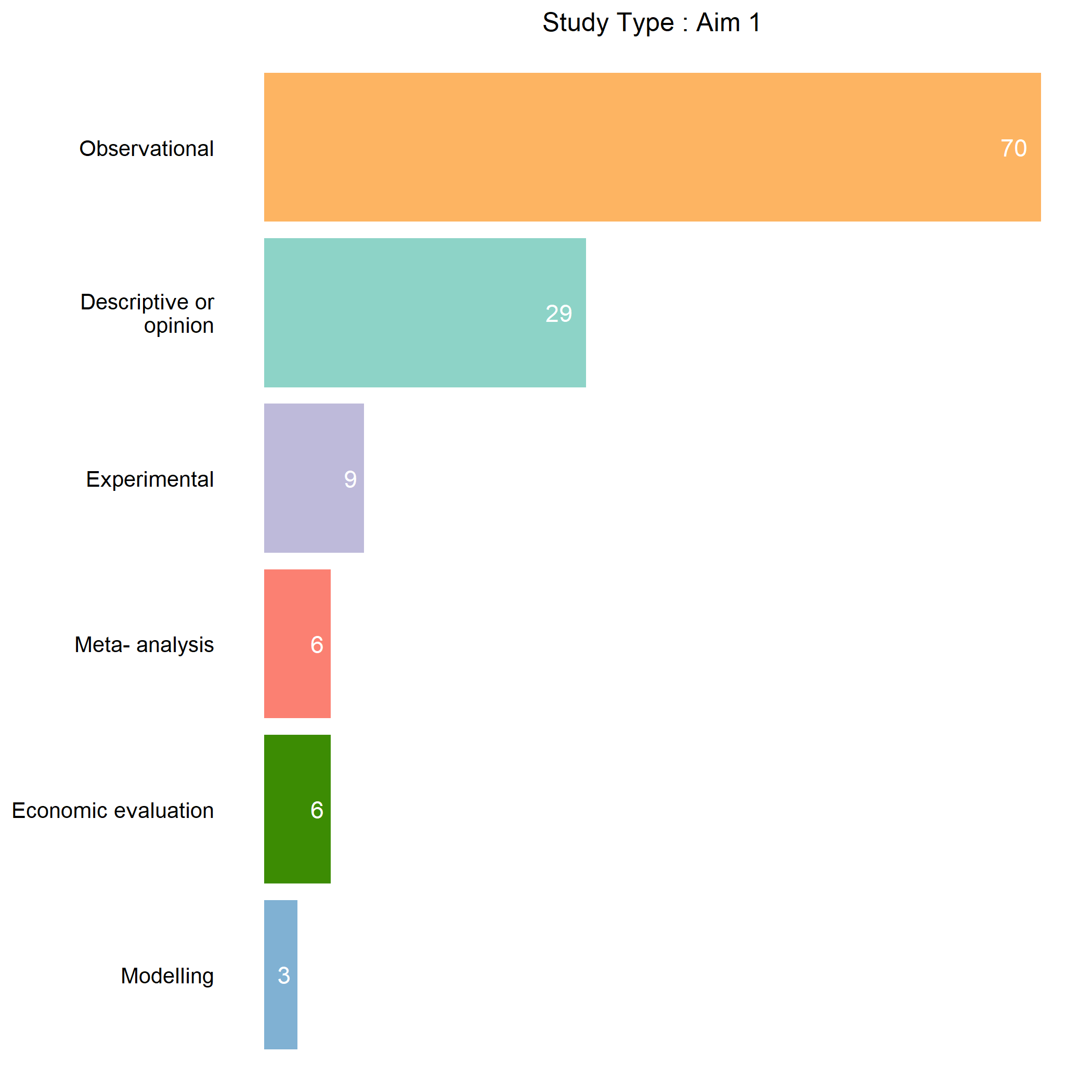 Figure 6 — Study type across Aim 1 sources.
Figure 6 — Study type across Aim 1 sources.
Community ownership. Of 90 rateable Aim 1 sources, 28 were rated “high”, 38 “medium” and 22 “low” for community ownership. Responses were rated “high” when principally initiated and implemented by one or more community-led organisations — including examples such as the Scarlet Alliance in Australia, GROOTS Kenya, the New Zealand Prostitutes Collective, the Uganda Community-led HIV/AIDS Initiative (CHAI), and organically-formed savings groups among female sex workers in Tanzania. Responses with a significant community-led element within a nonetheless predominately externally-framed programme were rated “low” — for example, the Sisters with a Voice programme in Zimbabwe, a top-down government programme with services delivered by sex workers but couched in an overall agenda and plan set by public actors.
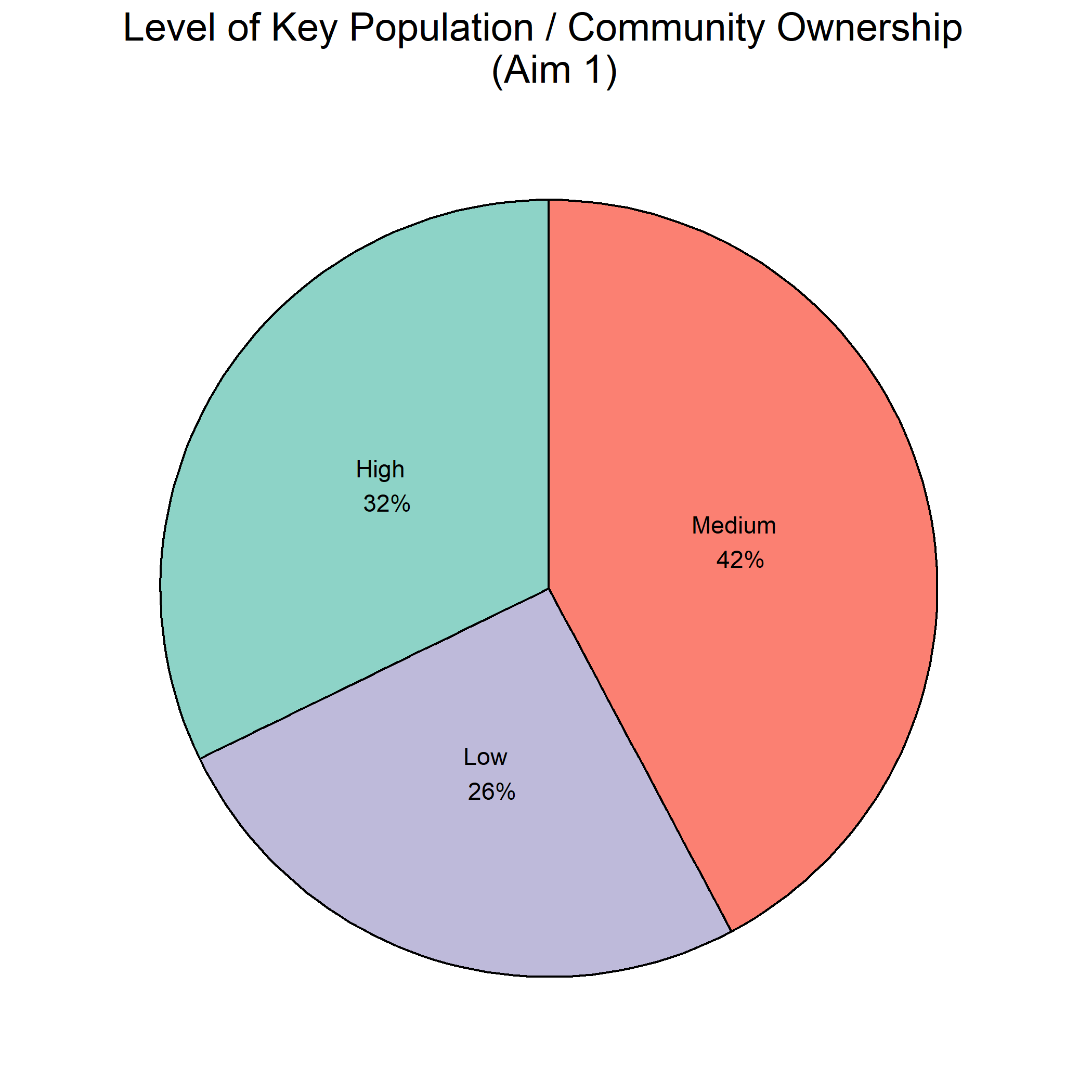 Figure 7 — Community ownership ratings for Aim 1 sources.
Figure 7 — Community ownership ratings for Aim 1 sources.
Types of responses. Despite the 30-80-60 commitment to a broad range of community-led responses (including societal-enabler programming), the literature is heavily focused on service-related responses. Three of the five most common observations on the focuses of community-led responses are delivery (n = 82), monitoring (n = 44) and advocacy (n = 38) for health services — 44% of all observations. Community-led responses related to legal and other structural determinants of health make up only 27% of the total.
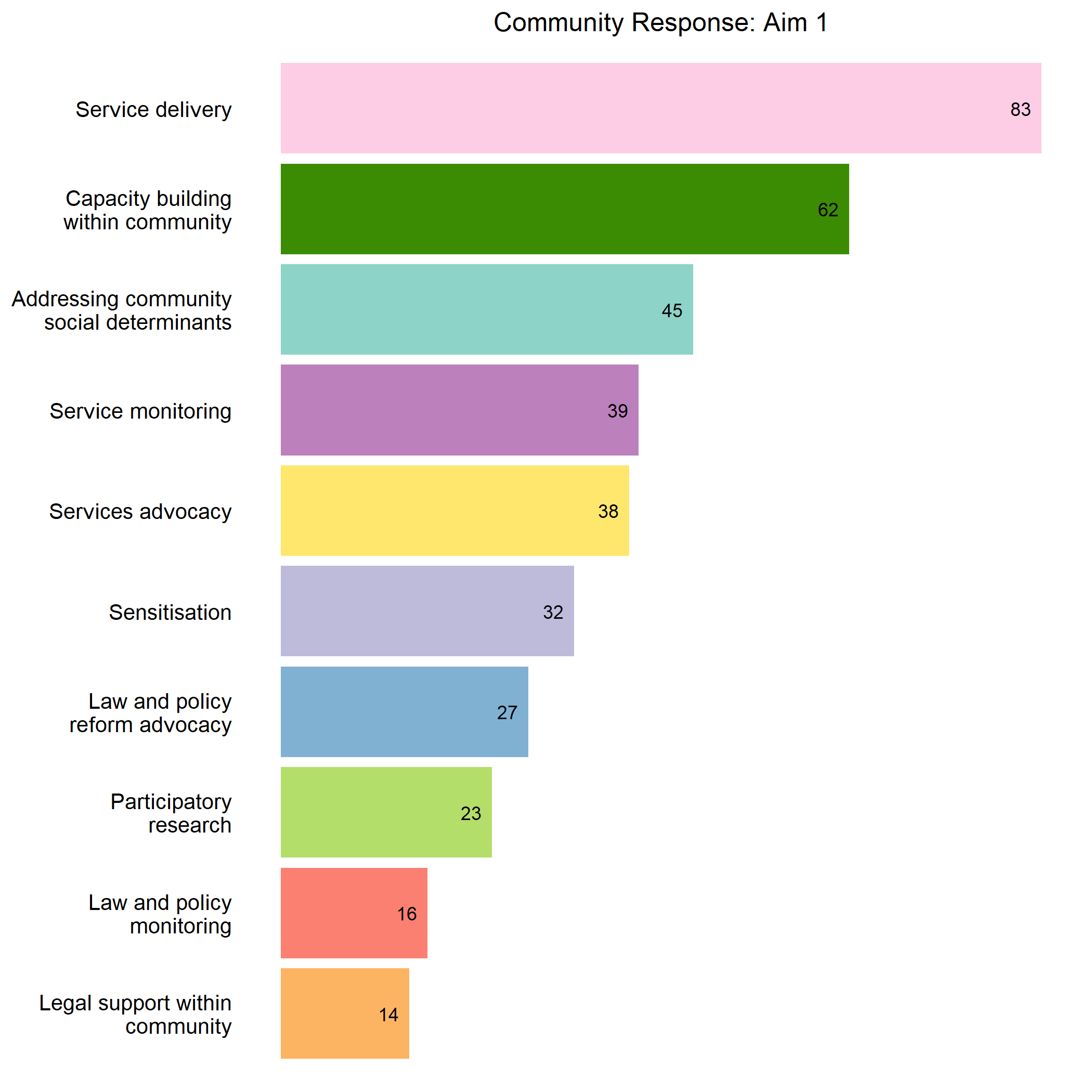 Figure 8 — Types of Aim 1 community-led responses.
Figure 8 — Types of Aim 1 community-led responses.
Priorities differ strikingly by community ownership level:
- “High” community ownership: 34% services / 30% legal determinants / 17% community capacity / 14% social determinants.
- “Medium” community ownership: 45% services / 17% legal determinants / 19% community capacity / 11% social determinants.
- “Low” community ownership: 54% services / 14% legal determinants / 17% community capacity / 10% social determinants.
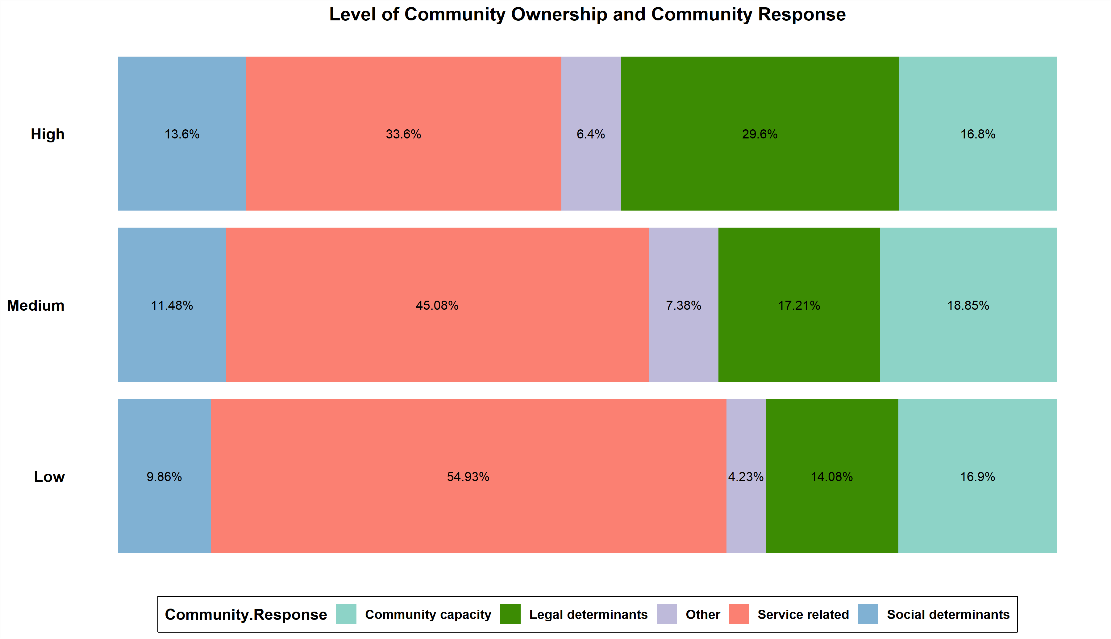 Figure 9 — Types of community-led responses by community ownership level.
Figure 9 — Types of community-led responses by community ownership level.
The clear conclusion is that community ownership affects the target of community-led responses: compared with external actors, communities consider legal and other structural determinants a higher priority and services a lower priority. This indicates that enhancing community ownership is one mechanism for ensuring on-the-ground programmes are in line with our global commitments — specifically, with the under-implemented commitment that 60% of programmes for advancing societal enablers be delivered by community-led organisations.
Benefits. All sources cite benefits to health — direct, indirect or mediated through the social determinants. Benefits are observed relatively evenly across prevention (n = 77), service access (n = 67), service quality (n = 67), and service demand, retention and utilisation (n = 63). Specific benefits in the form of reduced HIV incidence are recorded in 15 sources. None describe health benefits in terms of HALYs, QALYs or DALYs.
Nearly half of sources (n = 51) cited increased community capacity as a benefit; as many (n = 51) cited structural impacts such as equity; 31 sources cited both. Only four cited fiscal benefits such as costs averted or return on investment. Structural benefits include acquisition of new skills (especially for policy reform and the monitoring of laws, policies and practices), community empowerment through better-defined collective identity, and financial and housing security within responses that combine HIV with broader economic empowerment. A significant body of sources explores the benefits of community-led responses aimed toward reforming or sensitising external actors such as the police.
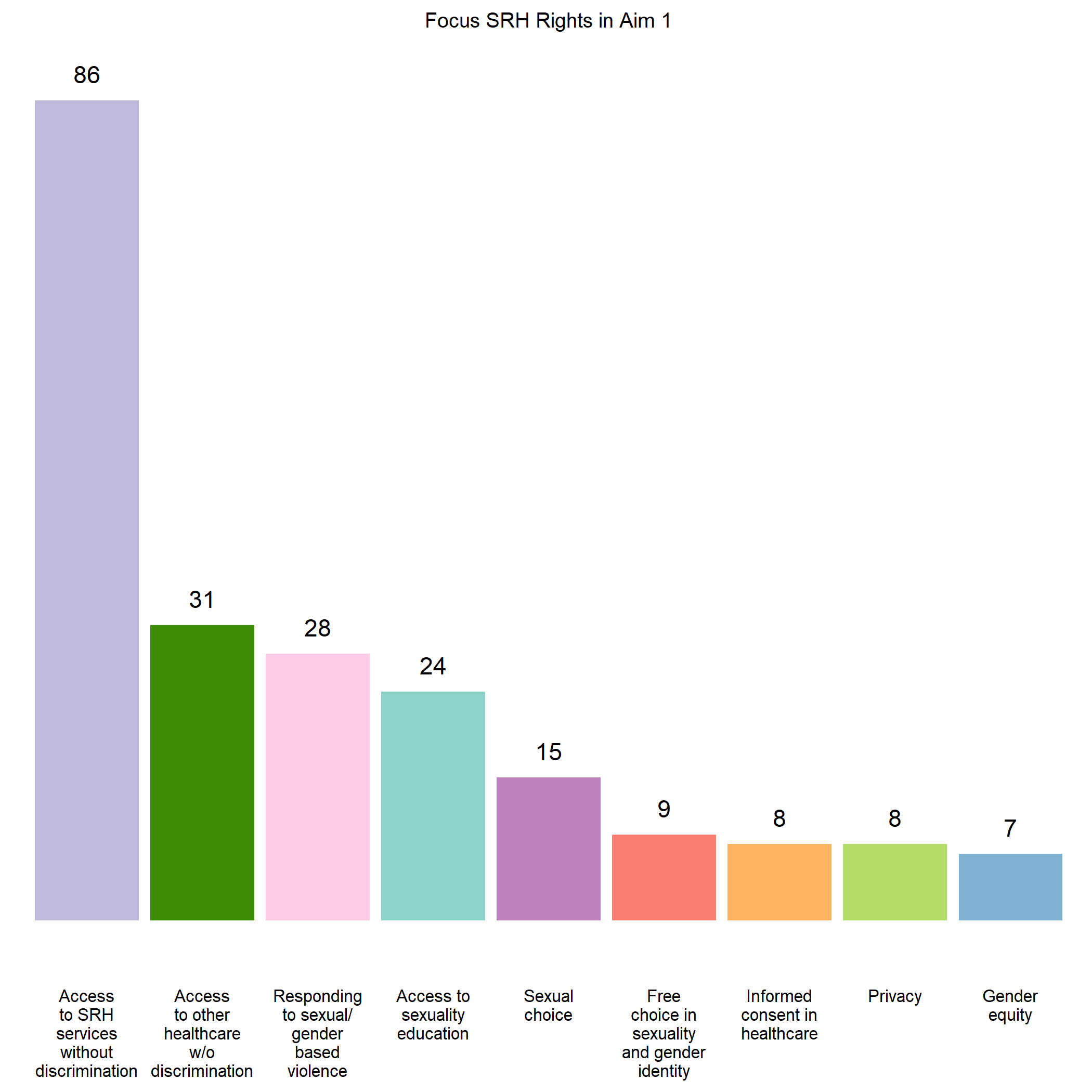 Figure 10 — SRHR rights benefits observed across Aim 1 sources.
Figure 10 — SRHR rights benefits observed across Aim 1 sources.
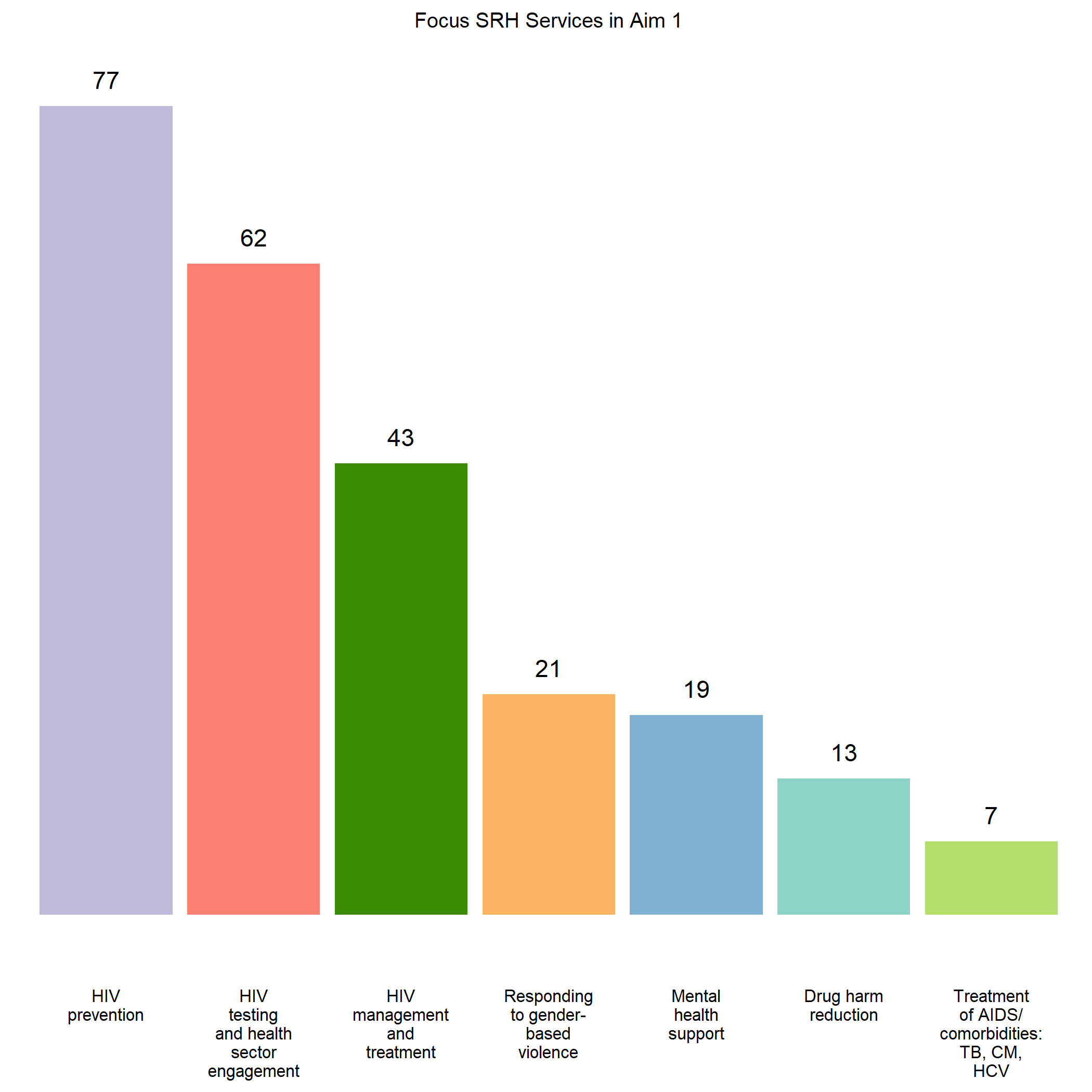 Figure 11 — SRHR services benefits observed across Aim 1 sources.
Figure 11 — SRHR services benefits observed across Aim 1 sources.
In total, the included sources cite 458 benefits associated with community-led responses, ranging across all areas of the 30-80-60 targets — testing and treatment, prevention, and societal-enabler programming. Despite this, there is an absence of literature on the current share of services and programmes delivered as part of community-led responses both globally and within individual countries, which — given the 30-80-60 quantitative targets — is a glaring research gap.
Funding and resourcing. Of 75 Aim 1 sources with extractable resourcing information, 34 cover both financial and other resource requirements, 29 cover only financial, and 11 cover only other. Only seven sources assess cost-effectiveness: four found the responses they explored to be cost-effective (encompassing a digital community-led prevention and legal-rights education response, and three responses focused on community-led distribution of HIV self-testing kits), two had mixed findings, and one found the response in question to be cost-ineffective (in an area with a low prevalence of undiagnosed HIV). Two studies identified cost-savings — both assessments of Avahan-initiative responses compared with government-run targeted interventions.
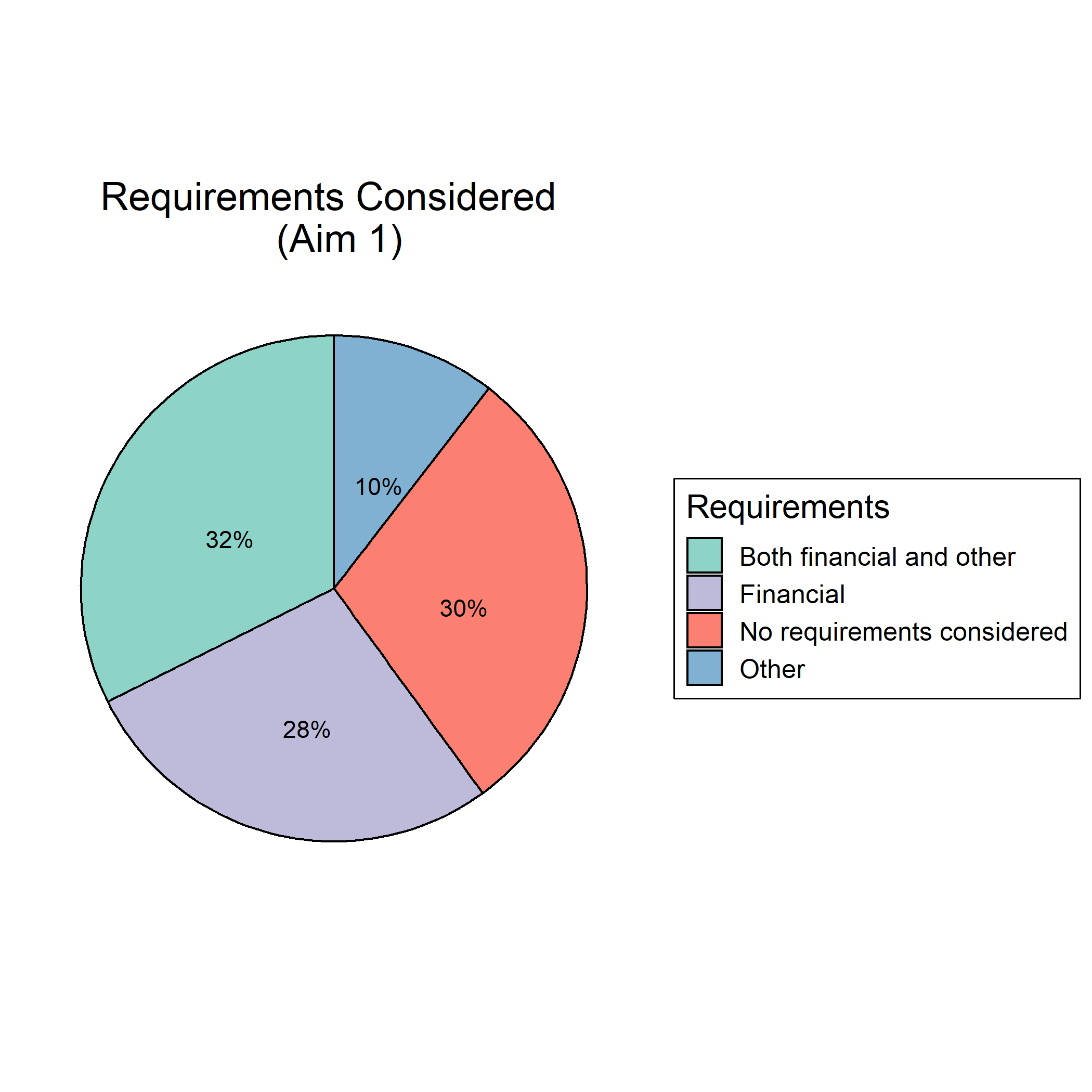 Figure 12 — Financial and other resource observations across Aim 1 sources.
Figure 12 — Financial and other resource observations across Aim 1 sources.
The specific resource-requirement figures found in the sources vary substantially — for example, US$1.5 per person helped per year for one sex-worker-targeted HIV prevention programme (cheaper than comparable programmes without a community-leadership component), US$38 per sex worker per year in another, and a total of US$285,065 (46% human resources, 23% HIV self-testing kits, 8% vehicles) in another. Funding sources identified varied across government, donors, user fees, and voluntary contributions from community members and implementers. Reliance on the time, money and other resources of volunteers is characterised in the sources as both a strength and a weakness — one study noting that “unpaid volunteers alone add an estimated 56 percent, on average, to CBO budgets in Kenya, Nigeria, and Zimbabwe”. Numerous sources raise resource requirements and funding as problems and challenges, with community-led organisations shuttering or reducing programmes due to insufficient and uncertain funding, and with narrow vertical interventions via social contracting or donor-driven priorities leaving community priorities underfunded and overall community capacity-building under-resourced.
Aim 2: legal determinants
Trends and settings. The distribution of Aim 2 sources across the last 15 years is more even than for Aim 1, reflecting both the accumulating emphasis on stigma, structural determinants and societal enablers, and the urgency raised by the significant harms criminalisation causes — alongside prevailing inaction despite this evidence. Of 267 Aim 2 sources, 59 explore a Love Alliance partnership country (Burundi is not among them), 88 explore similar settings, 91 focus on high-income settings coded as dissimilar, and 23 do not contain the full list of countries they explored. Populations featured: people living with HIV (n = 119), sex workers (n = 115), men who have sex with men (n = 81), people who inject and use drugs (n = 49), and transgender people (n = 45).
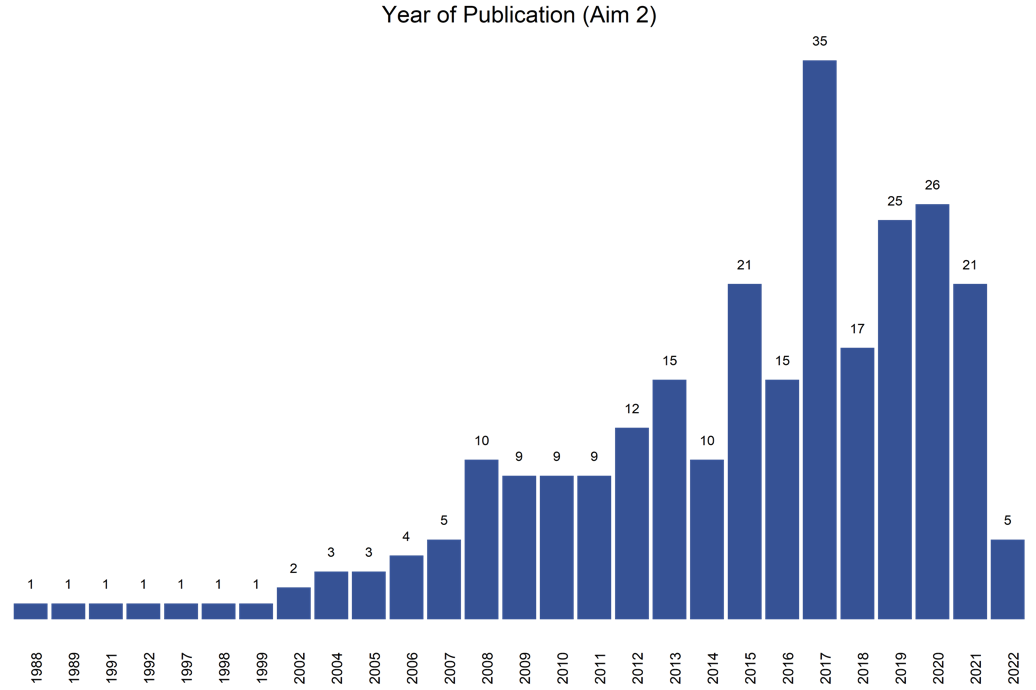 Figure 13 — Aim 2 sources by year of publication.
Figure 13 — Aim 2 sources by year of publication.
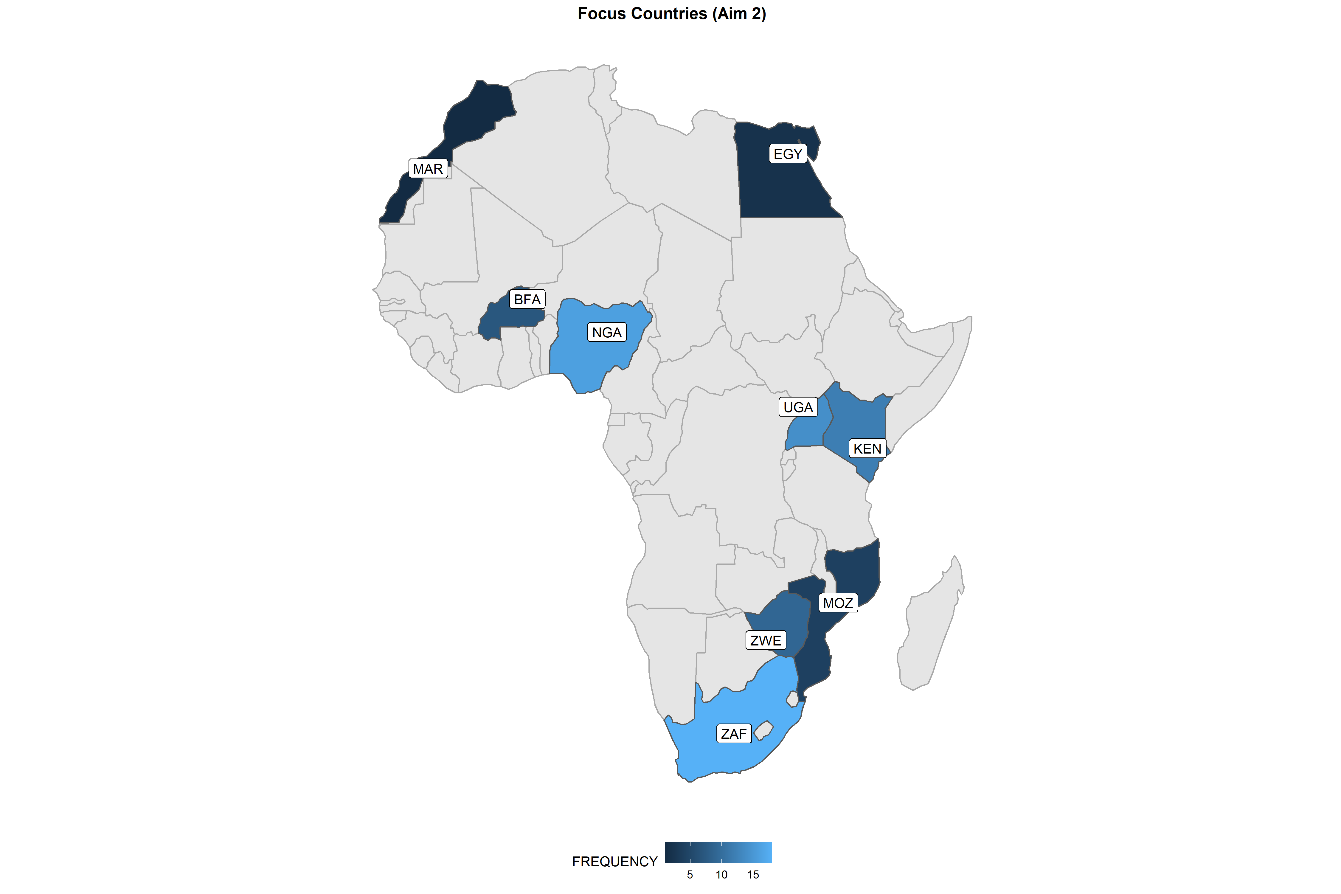 Figure 14 — Focus countries of Aim 2 sources.
Figure 14 — Focus countries of Aim 2 sources.
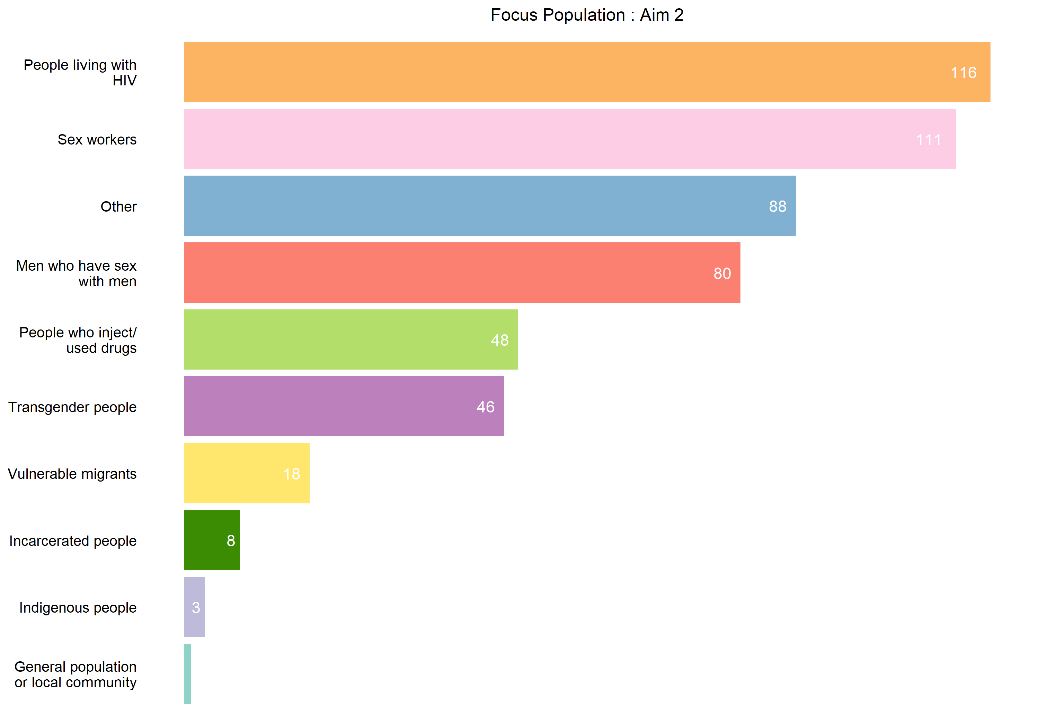 Figure 15 — Populations featured across Aim 2 sources.
Figure 15 — Populations featured across Aim 2 sources.
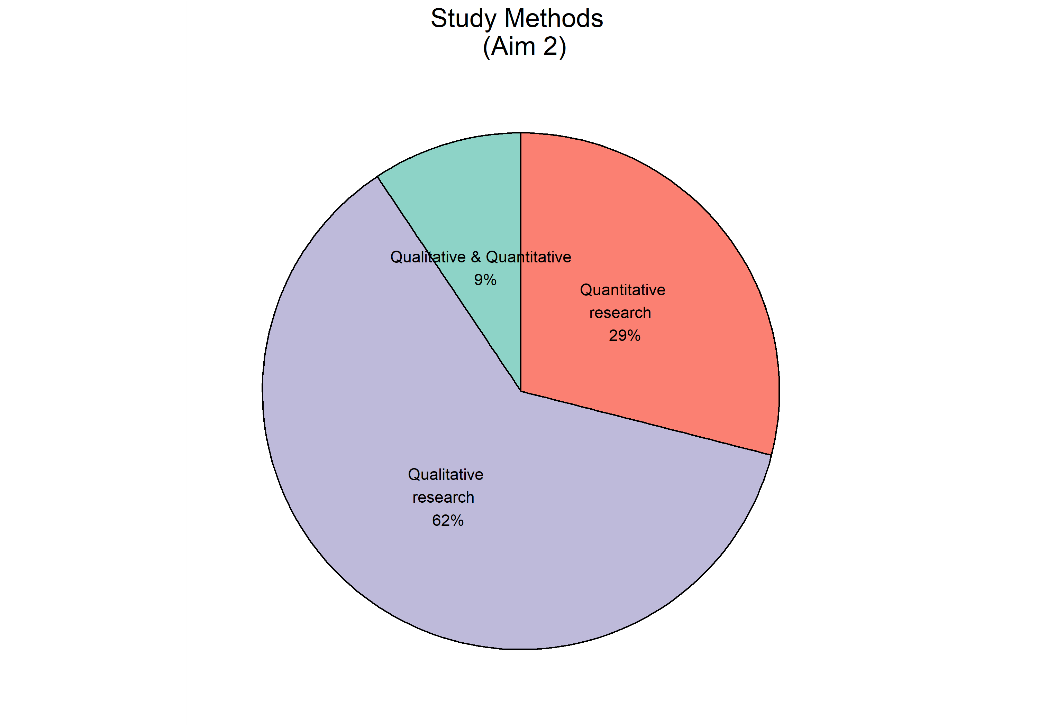 Figure 16 — Study methods used across Aim 2 sources.
Figure 16 — Study methods used across Aim 2 sources.
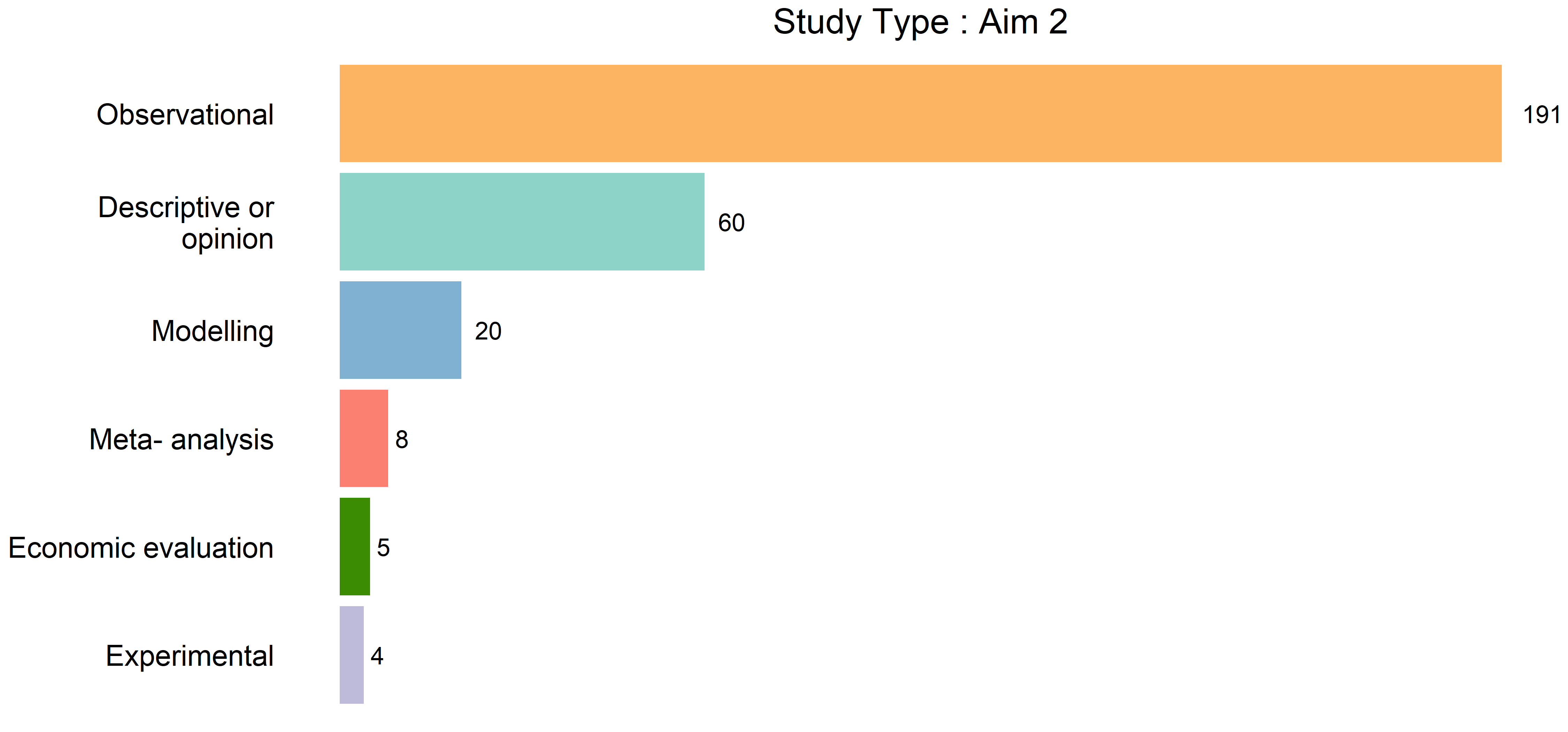 Figure 17 — Study type across Aim 2 sources.
Figure 17 — Study type across Aim 2 sources.
Negative vs positive legal determinants. The literature focuses disproportionately on the costs of negative legal determinants rather than the benefits of positive legal determinants. Only 19 sources observe only positive legal determinants, whereas 186 sources observe only negative legal determinants (with 63 more observing both). For both, discrimination, criminalisation and access to health services predominate across the sources.
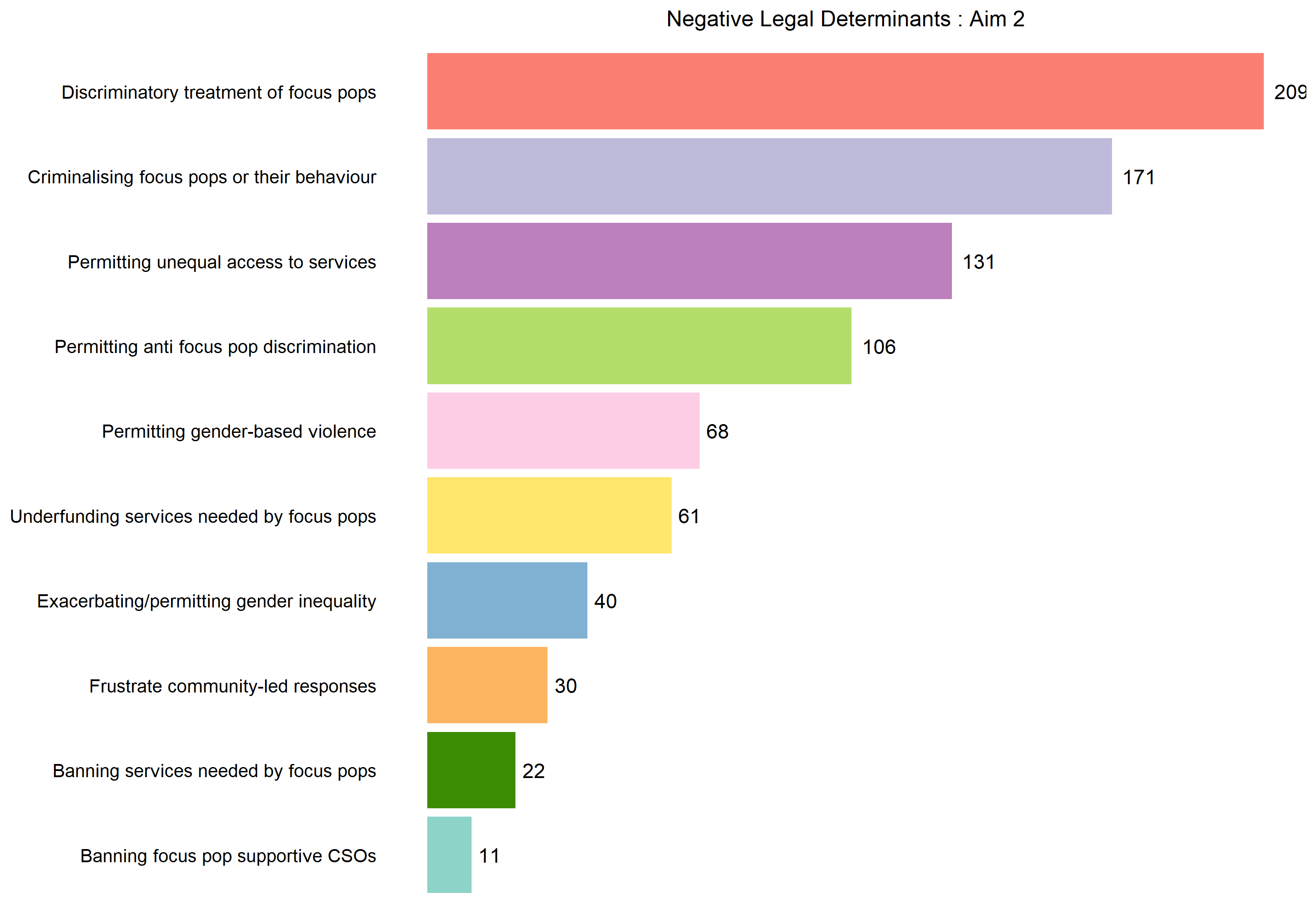 Figure 19 — Negative legal determinants observed across Aim 2 sources.
Figure 19 — Negative legal determinants observed across Aim 2 sources.
Costs of negative legal determinants. All but one of the included Aim 2 sources describe costs or benefits in terms of health impacts. None use HALYs, QALYs or DALYs. The most commonly described costs are the effects of criminalisation and discrimination on utilisation of and access to health services, including preventive and harm reduction services, and on the quality and acceptability of those services. Certain sources interrogate the legal soundness and reasonableness of criminalising HIV transmission by pointing to issues of consent, burden of proof, disclosure and prosecutorial discretion. The sources also associate various negative legal determinants with direct harms to health including greater risk of HIV, reduced status awareness and lower viral suppression; with gender-based and other interpersonal violence; with reduced access to housing, schooling and social services; and with private-actor discrimination including blackmail or reduced access to insurance. Specific pathways are frequently identified in extra-legal violence, harassment and extortion by police officers and other public officials, and in the inaccessibility of justice, legal services and complaint mechanisms. Certain sources focus on how coercive laws purportedly aimed at improving health not only contradict rights but also subvert the sought health objective — for example, Canadian laws criminalising HIV non-disclosure, which, although intended for prevention, in fact exacerbated transmission rates while disproportionately affecting already-marginalised people and women.
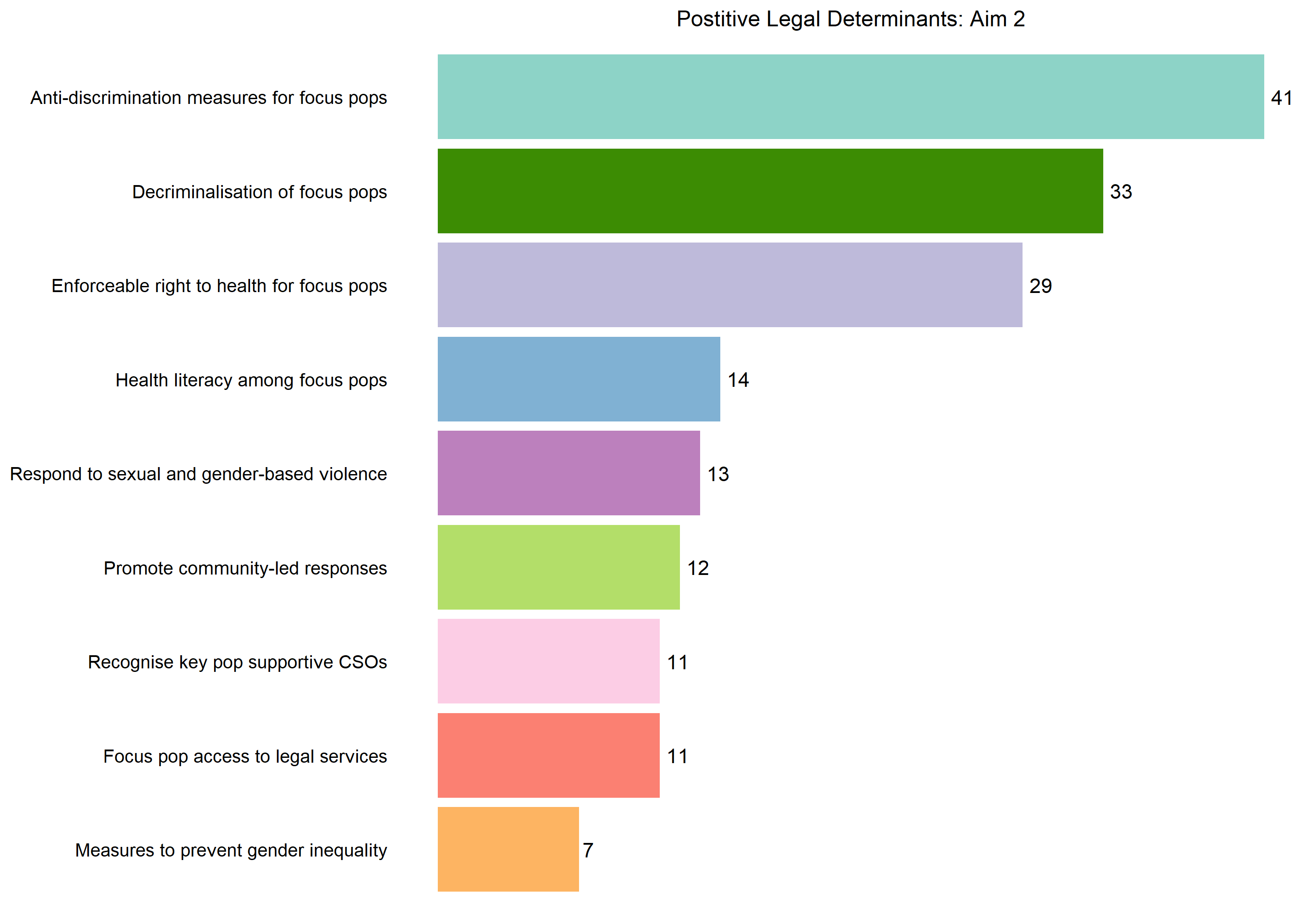 Figure 18 — Positive legal determinants observed across Aim 2 sources.
Figure 18 — Positive legal determinants observed across Aim 2 sources.
Benefits of positive legal determinants. Benefits are described in QALY and DALY terms in only three Aim 2 sources: an estimate of QALYs that could be averted through sex-work decriminalisation in three cities; an estimate of the QALYs averted through extending health insurance coverage to transgender care (reduced burden of HIV, depression, suicidal tendencies and harmful drug use); and an evaluation of DALYs saved per HIV infection averted across various structural interventions. Benefits of sex-work decriminalisation identified in the sources include measurable increases in safe-sex practices, declines in gender-based violence, and reductions in the incidence of HIV and sexually-transmitted infection. One study quantifies the economic benefits of decriminalisation in terms of income generated for sex workers per year and savings for the criminal justice and health systems. Other benefits of better laws and policies identified in the sources include reduced discrimination and privacy breaches; better insurance coverage; expanded access to harm reduction for people who use drugs including needle exchanges (with one source outlining preventive value within closed settings and another exploring the effect of a law prohibiting police interference with drug harm reduction services); and the integration of peer and community-based action in HIV programmes.
Certain sources characterise legislative reform as not always itself enough. Legal reforms can be meaningful only with access to adequate and simplified legal information and strong redressal mechanisms; two studies show that laws legalising drug harm reduction were, although beneficial, insufficient in themselves when set against police discretion, stigma and competing laws criminalising drug use; and another series of studies explores how discriminatory practices and stigma institutionalised through criminalisation will not dissolve merely as a result of partial or full decriminalisation. A handful of sources — mostly focused on British Columbia — analyse how non-criminalisation of sex work alone is not sufficient when the broader legal environment remains hostile to the labour rights and business practices of sex workers.
Cross-cutting results
Our results indicate a reasonable degree of correspondence and mutuality between the two sets of evidence mapped pursuant to each aim: 13% of Aim 2 sources (n = 39) and 43% of Aim 1 sources (n = 51) include at least one cross-cutting variable, so 90 sources speak to both aims.
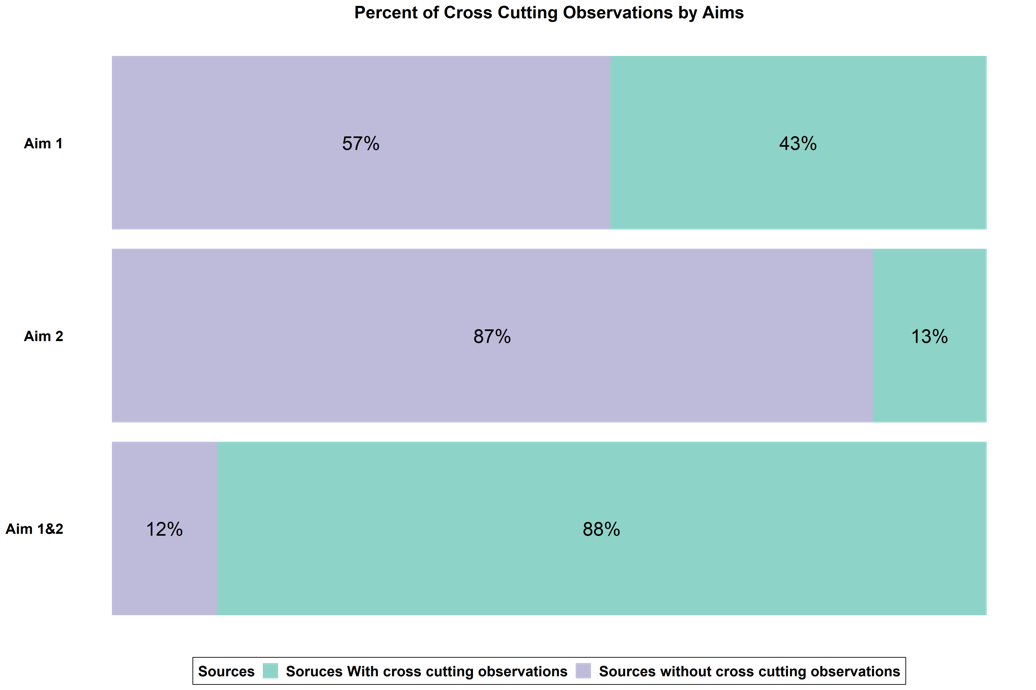 Figure 20 — Cross-cutting sources across Aim 1 and Aim 2.
Figure 20 — Cross-cutting sources across Aim 1 and Aim 2.
Community-led responses for improving the legal determinants are explored in 51 Aim 1 sources. Of these, 31 sources include discussion of community-led sensitisation of police, healthcare providers and others as a way of shifting practices; 28 show community-led advocacy for law and policy reforms; 16 explore efforts at law and policy monitoring; and 14 feature the provision of legal support within the community. Sensitisation activities are the most commonly pursued community-led response for shifting legal determinants, encompassing both formal training of individual officials and the creation of institutional relationships, with benefits including reductions in police violence and better access to services.
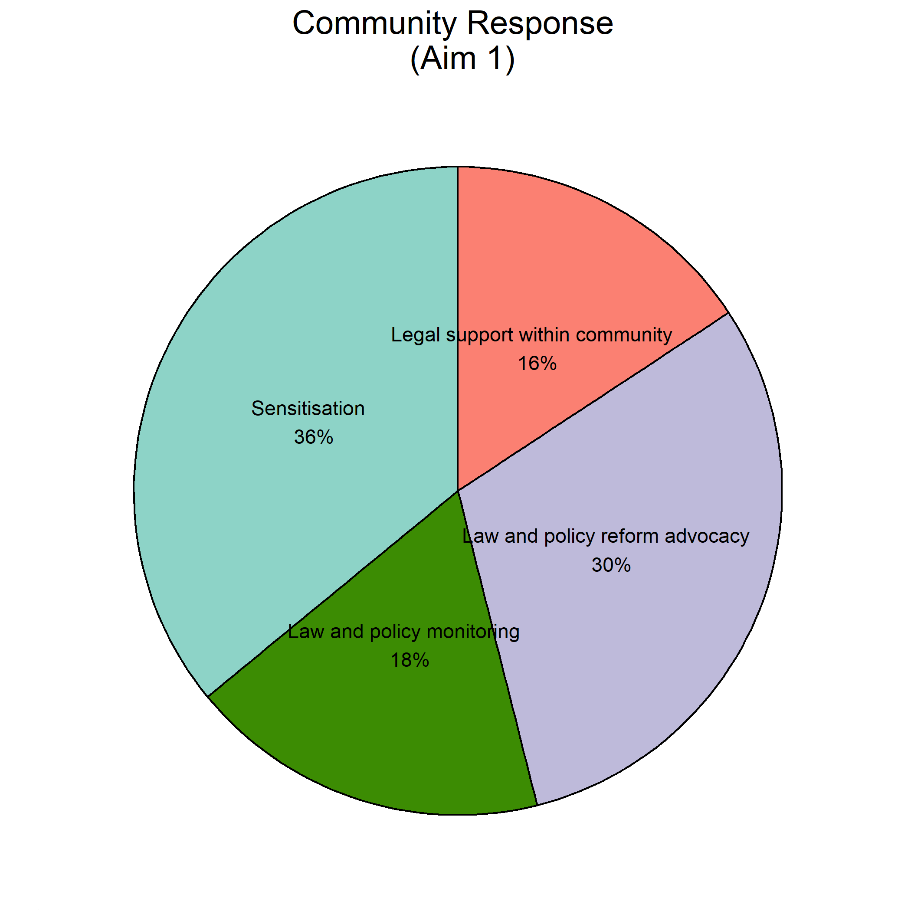 Figure 21 — Community-led efforts for better laws across cross-cutting Aim 1 sources.
Figure 21 — Community-led efforts for better laws across cross-cutting Aim 1 sources.
Case study — the New Zealand national needle exchange and DIVO. The legislation enabling New Zealand’s national needle exchange legalised and funded the provision of needles and syringes via local organisations led by people who inject drugs, which could apply for recognition. One of these, the Dunedin Intravenous Organisation (DIVO), not only provided the service it was contracted for but also went beyond it — conducting research, forming cross-organisation ties, presenting at conferences, publishing community literature, building up community capacity, and lobbying to reform institutional and law-enforcement practices within prisons and the police squad. The source presents a positive feedback loop of community-led response leading to law reform that, in turn, promoted yet more community-led responses including those aimed at improving the legal determinants of health.
Case study — the New Zealand Prostitutes Collective (NZPC) and decriminalisation. From its founding, NZPC was caught between a police force seeking to enforce criminalising laws and a Ministry of Health that funded the organisation to provide health-promoting and harm-reduction services. Its responses to improve the health of its community were frustrated by police action. Following agitation by NZPC, the broader community and allies, legislation decriminalising sex work was passed. This law removed an obstacle to NZPC’s responses for community health, enabled sex-worker collectivisation and promoted further community involvement in shaping health policy.
Laws, policies and practices promoting or frustrating community-led responses are explored in 39 Aim 2 sources. Related observations occur in only 23% of Aim 2 sources, but they are disproportionately represented among the sources on positive determinants (40%) compared with those on negative determinants (13%).
Positive laws, policies and practices promote community-led responses by directly recognising them and by lifting direct and indirect barriers to their operation — for example, by according legal status to activities such as harm reduction or testing services undertaken within community-led responses; by providing legal personality to community-led organisations or creating partnerships with communities of key and vulnerable populations; and by providing dedicated funding for needed services and capacity building. Anti-discrimination measures, decriminalisation of sex work and legalisation of drug harm reduction services can enable community-led responses to build and act on the capacity and legal literacy needed to enforce these provisions.
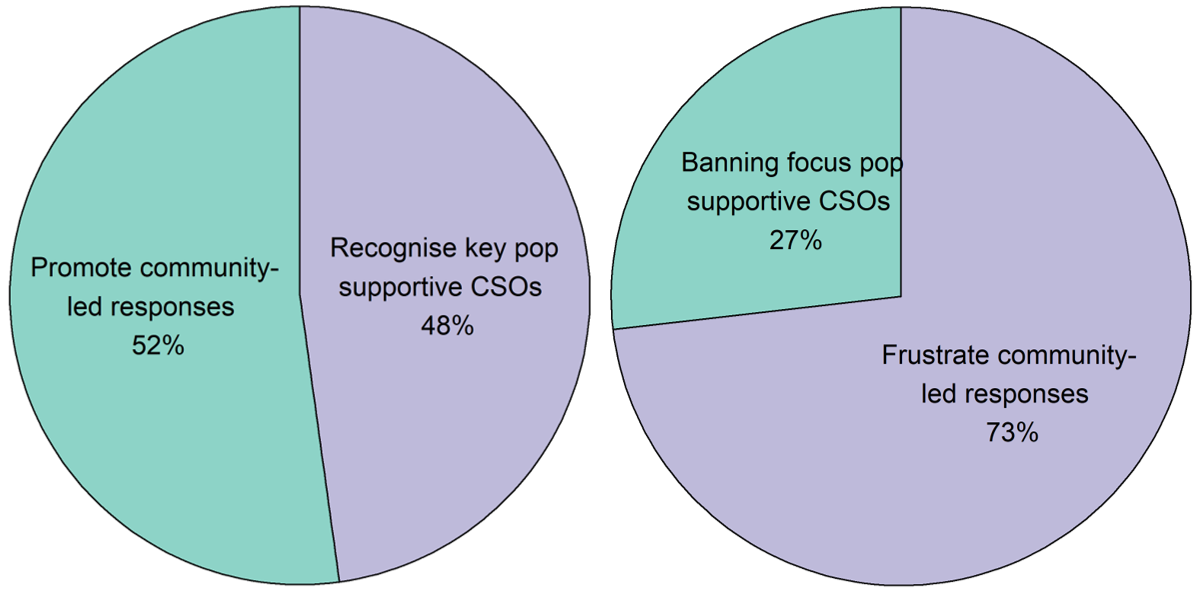 Figure 22 — Laws, policies and practices that promote or frustrate community-led responses.
Figure 22 — Laws, policies and practices that promote or frustrate community-led responses.
Negative laws, policies and practices frustrate community leadership and ally civil society through direct prohibition or burden on community-led and ally civil society organisations (frequently deeply entangled with the criminalising, discriminatory and punitive laws applied toward members of key and vulnerable populations), indirect barriers (e.g. funding application criteria structured toward actors with more resources and capacity than community-led organisations typically have), and criminalising, punitive and discriminatory measures aimed at key and vulnerable populations themselves. For example, “anti-drug drive operations” in Dhaka not only caused direct harm by provoking risk injection practices and extrajudicial police violence but also frustrated community-led responses by exposing outreach workers to police violence and obstructions, and by dispersing those they were seeking to help. The successful community-led response by GROOTS in Kenya aimed at protecting vulnerable women and responding to HIV by upholding property rights was frustrated by fragmented land laws and a lack of integration between community-led mechanisms for securing land tenure and the formal legal system.
Discussion
Our main findings can be summarised across three groups.
Cross-cutting: (1) there is a large body of literature relevant to both aims, growing rapidly for Aim 1 and more stable for Aim 2; (2) coverage is sufficient for settings the same as or similar to the Love Alliance countries; (3) for both aims, there is less literature on the concerns and situations of transgender people and people who use drugs.
Aim 1: (4) sources substantiate the already well-evidenced benefits of community-led responses but are disproportionately focused on short-term and small-scale interventions; (5) the degree of community ownership appears to affect the priorities and aims of community-led responses; (6) as community ownership increases, responses become more diverse and less narrowly focused on service delivery; (7) the literature focuses on responses with less community ownership and therefore provides only a partial evaluation of community leadership’s potential; (8) few sources describe benefits in terms of cost-effectiveness or amenable to economic evaluation; (9) few studies provide precise measures of financial resource requirements, and those that do vary substantially given the wide variance in types of response and settings; (10) reliance on underpaid or unpaid labour from volunteers within the community was identified as a common resource; (11) many sources describe resource requirements in terms of the challenges of unreliable, insufficient or overly prescriptive funding.
Aim 2: (12) sources more commonly feature laws, policies and practices that negatively impact SRHR; (13) the most common pathway for negative impact is discrimination and criminalisation, and the most common pathway for positive impact is anti-discrimination and decriminalisation; (14) negative laws, policies and practices are characterised as undermining access, availability and quality of health services and as undermining health-promoting behaviours; (15) positive laws, policies and practices highlight the limitations of isolated reforms and the need for concerted approaches of mutually-supportive legal reforms and broader societal interventions.
Mutuality: (16) there is a reasonably high degree of mutuality between the two sets of sources; (17–19) Aim 1 and Aim 2 cross-cutting sources indicate that community-led responses are often aimed toward and meet with success in improving legal determinants, while the legal environment can be both a barrier to and an enabler of community leadership. Taken together, these sources indicate a literature that explores, albeit infrequently overtly, the mutuality of the 10-10-10 and 30-80-60 targets.
Policy and advocacy implications
The included sources demonstrate the urgency of addressing the harms of criminalisation and other negative laws, as well as the benefits of implementing laws to protect against discrimination and to decriminalise people and their behaviours. At the same time, the literature shows the limitations of isolated reforms that target only a single component of complex and intersectional forms of legal, extra-legal and societal marginalisation and discrimination. In the absence of action, health is harmed, health services are impaired, and community-led responses are obstructed and frustrated. Accordingly, this review demonstrates how fundamental attention to the legal determinants is for realising the full potential of community-led responses and ensuring progress on ending HIV and preventing deaths from AIDS.
Our review confirms the interrelationship between investment in community leadership and progress on the societal enablers. Our findings of the mutuality of studies relating to the two sets of targets can be cited to confirm the premise of the “60” target — that communities need to lead on delivering programming for the societal enablers. Community-led responses are also of impact in improving the legal determinants, and such improvements are a common aim and outcome.
This review supports investment in and advocacy for community-led responses to HIV and related SRHR challenges. All sources cite benefits to health; community leadership and ownership also benefit the prioritisation and design of responses by ensuring they target areas of greater community need and grapple with the challenges posed by preventing, mitigating and reforming bad laws. Global and national responses that aim to meet the challenge of HIV with sufficient ambition need to have community leadership at their heart and to promote the highest level of community ownership attainable.
Meeting this challenge requires financial investment from countries and from global funders. The research on community-led responses is characterised by frequent reporting on the challenges and pitfalls of uncertain and inadequate funding. These funding challenges make delivering services or programming challenging, difficult or impossible; more subtly, they can warp the character of the community-led response by requiring communities to fit the prescriptions and reporting requirements of funders rather than the needs and processes preferred and most suited to the communities themselves. High-quality and high-ownership community-led responses require capacitation and organisational development over the long-term, which makes sustained and predictable funding essential. In agreeing to the 30-80-60 targets, the countries of the world also agreed to sustainably financing community-led organisations and networks. There is a pressing need to hold countries and funders to account in fulfilling this commitment.
A related challenge is the overreliance on community voluntarism. Shifting funding and programming to community-led responses as a means of exploiting their passion to extract free labour and other resource commitments from already-marginalised populations is wrong. The benefits of community leadership should, instead, be located in the leadership of the communities — in the immense added value of directing resources to people who know their needs and their capacities best to creatively advance responses to HIV and related SRHR challenges. Community-led organisations need to be resourced well enough that roles which merit compensation and wages receive them.
Research implications
The determination, design and implementation of all research agendas, programmes and studies should be community-led. As this review establishes, the priorities of interventions shift depending on the degree of community ownership over them; the same will apply for community-led research. The research gaps identified below should therefore be understood as potential priorities, with determination of actual priority left to relevant community-led organisations and networks.
-
A typology of community-led responses. Community-led research delineating a typology of responses — extending and formalising this review’s distinction based on community ownership, and categorising responses by longevity, scale, type of issues, interventions encompassed, and structures of the community-led organisations or networks involved. This will assist in assessing future and past responses with greater granularity and help identify the characteristics — low community ownership, short duration, small scale — that may hinder effectiveness.
-
The financial and resource requirements of community-led responses and their overall share within the HIV response. Further review of existing datasets and investigation of past and present responses, supported by greater transparency and disaggregated reporting by funders and implementers on financial resource requirements and the share of programming delivered by community-led responses. This will help to determine the proportion of services and programming for the HIV response being delivered as part of community-led responses in line with the 30-80-60 targets.
-
Research on and investment in large-scale, long-term, and maximally community-owned responses in diverse regions, including those of Africa. This is needed to determine the relative cost-effectiveness of community-led responses and to unlock the full potential of community leadership in settings that criminalise or permit discrimination against key and vulnerable populations. Preliminary research will be needed to establish the minimum scale and duration needed to estimate cost-effectiveness for different types of community-led responses.
-
A mixed-methods package. The above priorities could be packaged together in a mixed-methods study comprising a systematic review and meta-analysis as well as econometric evaluations, cost analysis and qualitative interviews — with scope extended beyond the present review’s focus on health outcomes and determinants of health, to more fully demonstrate the broader positive externalities of community-led responses.
-
How positive and negative legal determinants enable or frustrate community-led responses. Law-reform advocacy could be strengthened by further evidence substantiating the connection between an effective HIV response, community leadership, and circumstances of non-discrimination and decriminalisation — delineating causal links, effect sizes, and the types of legal determinants and overall frameworks that enable and support community-led responses.