How Law Reform and Better Investment Enable Highly Effective Community-led Responses for SRHR

Juliette McHardy and Agrata Sharma, O’Neill Institute’s HIV Policy Lab. Produced December 5, 2022.
The report distils the actionable findings of the scoping review, itself developed through an extended programme of consultation with Love Alliance partners, bilateral partners and civil society.
Summary
This report is focused on how strong community leadership and better laws and policies act as positive determinants of sexual and reproductive health and rights. There is a strong evidence base on the benefits to health that result from community-led responses and better laws and policies. Improving laws and policies is particularly crucial for realising the full potential of community-led responses in advancing sexual and reproductive health and rights. At the same time, community-led responses are an important means of reforming and reinforcing reforms in law and policy as well as realising progress on the broader determinants and enablers of sexual and reproductive health and rights. To unlock these mechanisms for change, more and better investment in community-led responses is needed. Inadequate, unreliable, and overly prescriptive funding poses a barrier to the high-quality and high-ownership community-leadership required in the responses to our world’s sexual and reproductive health challenges.
Overview
The Global AIDS Strategy 2021-2026 recognises that ending inequalities affecting key and vulnerable populations is essential to the HIV response. It makes this aspiration concrete in the 10-10-10 targets for reducing the societal barriers to the realisation of sexual and reproductive health and rights. At the same time, the 30-80-60 targets aim to uphold community-led responses as indispensable societal enablers of the same rights. The two sets of targets are interlinked with community-led responses needed to remove impediments to HIV responses and with progress on the societal enablers — in particular, better legal environments — also a facilitator of community leadership.
Given the explicit connection drawn between empowered community leadership and progress on societal enablers in the Global AIDS Strategy, the Love Alliance commissioned a scoping review to take the HIV response as a case study for looking at how, across sexual and reproductive health, better investment in community-led responses and reforms to rights-denying laws can unlock progress. In the scoping review, we aimed to:
- Outline evidence on resource requirements and benefits of community-led responses for sexual and reproductive health and rights (aim one).
- Put this evidence into context with a mapping of the literature on the benefits or costs of good or bad laws, policies and practices (aim two).
We approached these aims with a systematic scoping review (the Review) of scientific and grey literature supported by engagement and consultation with community partners and experts. A particular focus was the “60” of the 30-80-60 — i.e., 60% of all programmes for the achievement of societal enablers are to be delivered by community-led organisations.
Definitions
Determinants of sexual and reproductive health and rights. By definition, “determinants of health” are neutral in their meaning. They are conditions in the environments of people that affect their health or, in this case, their sexual and reproductive health and rights. These determinants can be harmful or beneficial, as well as both harmful and beneficial.
Societal enablers of the HIV response. Within the global HIV response, societal enablers are pathways for removing impediments to HIV prevention, management and care including improved legal environments, reduced stigma and discrimination, and action to overcome gender inequalities and gender-based violence. Community leadership is also a societal enabler of the HIV response.
Legal determinants of sexual and reproductive health and rights. The legal determinants comprise laws, policies and practices that promote, fail to support, or undermine sexual and reproductive health and rights including rights-affirming and non-discriminatory measures as well as measures that are criminalising, discriminatory or stigmatising. Harms result from both actively discriminatory and criminalising laws, policies, and practices as well as the absence of laws and policies for protecting and fulfilling rights. The legal environment can be both an impediment to and enabler of community-led responses.
Key and vulnerable populations. Key and vulnerable populations comprise those people who are, with respect to a particular sexual and reproductive health challenge, at an elevated risk and whose needs and rights should be centred and upheld as part of the public health response. Within the context of HIV, key populations include people living with HIV, men who have sex with men, transgender people, people who inject drugs, sex workers and their clients, while vulnerable populations and marginalised people include, at minimum, women and girls — in particular adolescent girls and young women — as well as incarcerated people and others living in closed settings.
Community-led responses. Community-led responses comprise a diverse set of interventions carried out at varying scales and levels but are all informed, implemented and determined by communities for their own members. Communities ensure their own sexual and reproductive health and rights by advocating for, delivering, designing and monitoring health services, designing, implementing and participating in research, and monitoring and advocating for human rights accountability as well as reforms to laws, policies and practices. Not all responses involving community members or community-led organisations are, themselves, community-led, even if described as such, but, equally, a response may still be community-led even when not termed as such.
The 10-10-10 and 30-80-60 targets
The 10-10-10 targets are aimed at the societal enablers of the HIV response:
- Less than 10% of countries have punitive legal and policy environments that lead to the denial or limitation of access to services.
- Less than 10% of people living with HIV and key populations experience stigma and discrimination.
- Less than 10% of women, girls, people living with HIV and key populations experience gender-based inequalities and all forms of gender-based violence.
The 30-80-60 targets are aimed at community leadership in the HIV response:
- 30% of testing and treatment services are community delivered.
- 80% of HIV prevention services are community delivered.
- 60% of programmes supporting the achievement of societal enablers are community delivered.
Theory of Change
Problem identified. Responses led by those communities most affected by sexual and reproductive health challenges are effective at ensuring access to quality health services and improvements in legal determinants but are underfunded, underutilised and often stunted by inhospitable or even punitive legal environments that deny them their rights and ability to organise.
Process of change. The principal mechanisms for change will be an escalation of the degree and quality of community leadership over responses to sexual and reproductive health challenges alongside a shift away from framings of sexual and reproductive health that subvert or minimise the importance of rights-based approaches. By acting on both of these sets of mechanisms, a mutually reinforcing cycle of improvement will occur by which better law and policy environments will facilitate community-led responses while community-led responses advance the implementation of reforms to law and policy.
Needed inputs. One of the key inputs to catalyse this process for change is investment in community-led responses and other programmes for shifting laws, policies and practices that impede and fail to protect the exercise of sexual and reproductive health rights. This requires investment of sufficient scale, duration and certainty that is delivered without any undue conditions which deprive communities of genuine leadership.
The value of community-led responses
In determining the agenda
A community-led response’s distinguishing value lies in the community’s leadership over it and the ways this leadership is expressed in a response’s chosen objectives, design and implementation. The Review found that responses differ in ways needed under our global HIV commitments when communities have greater degrees of ownership over their responses. Despite this, the literature on community-led responses eligible for inclusion in the Review is heavily focused on responses for and concerning services (see Figure 1).
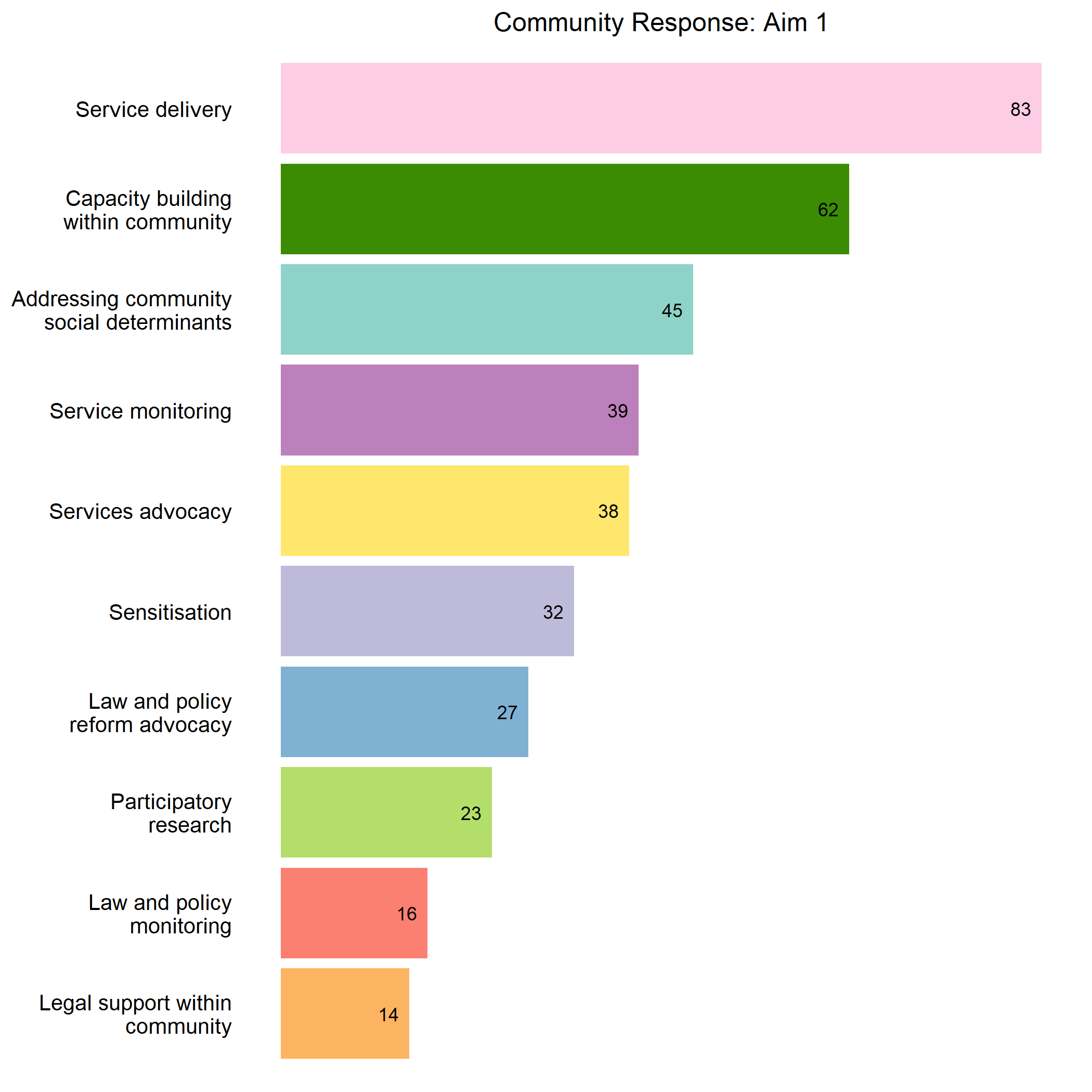 Figure 1 — Community-led responses by type (Aim 1 sources).
Figure 1 — Community-led responses by type (Aim 1 sources).
This shifts when there is a higher degree of community ownership within and over a community-led response. The Review indicates that, compared with external actors, communities consider legal and other structural determinants a higher priority and services a lower priority. Specifically, while a similar proportion of responses were targeted toward community capacity (17%, 19%, 17%) and the social determinants (14%, 11%, 10%) across all three levels of community ownership, there are significant differences when we compare the proportion of those aimed at legal determinants (30%, 17%, 14%) — see Figure 2.
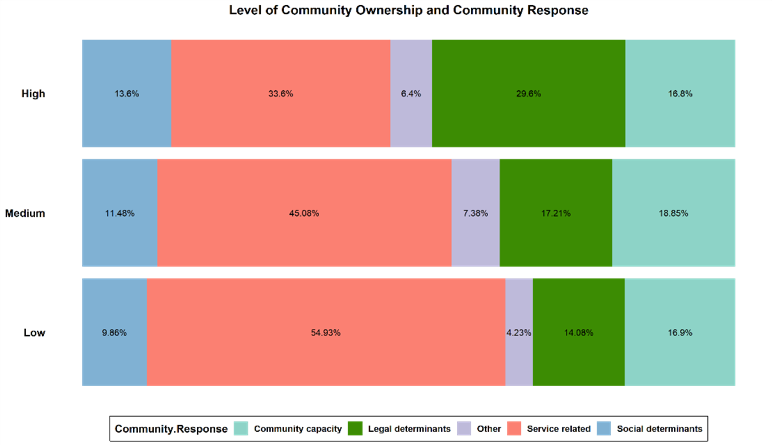 Figure 2 — Types of community-led responses split by level of community ownership.
Figure 2 — Types of community-led responses split by level of community ownership.
Accordingly, one of the benefits of community ownership is ensuring on-the-ground programmes are in line with our global commitments. Achieving the 30-60-80 targets requires accelerating implementation of the relatively under-implemented commitment that 60% of programmes for advancing societal enablers be delivered by community-led organisations. Funders, state or otherwise, must be cautious when dictating the priorities for such initiatives and let the community take the lead on both program design and implementation.
Deep Dive 1 — Community Ownership. In the Review, the Sonagachi initiative was rated as having “high community ownership”. This sex worker-led response focused on individual and community empowerment and structural changes. By contrast, despite having elements of community leadership and service delivery by sex workers, the Sisters with a Voice programme in Zimbabwe was categorised as having “low community ownership” due to being a top-down government programme with the overall agenda and plan set by public actors, based out of clinical settings, and supervised by non-sex worker outreach workers.
Part of ensuring community-led responses are truly owned by the affected communities is work on promoting both general and working definitions of the community leadership needed and their inclusion in clear coordinating mechanisms or terms of reference between funders and relevant community-led organisations.
Regarding societal enablers and legal determinants
The benefits of community-led responses described in the literature are diverse. They include the acquisition of new skills within the community, especially ones relevant for policy reform or the monitoring of laws, policies, and practices. Process benefits attributed to community-leadership include the effective development and timely implementation of relevant and efficient programs. Another commonly described benefit is community empowerment through a better definition of community identity and its effectiveness to enable structural changes. Financial and housing security are also cited as benefits of community-led responses within four sources that explored economic empowerment and social determinants.
Case Study 1 — Pragati Initiative. The “high community ownership” Pragati Initiative exemplifies the holistic impact of community-led responses for the societal enablers and legal determinants. It showcases improvements to the health-related outcomes of key populations and increases in their capacity to protect their own bodily integrity and autonomy as a result of access to reproductive health services and addiction services and the gender-based violence prevention. At the same time, access to microfinance and crisis response facilities improved broader social determinants of health.
A particularly prominent benefit of community-led responses is in shifting the legal determinants of sexual and reproductive health by reforming law and policy or by improving its implementation. For example, a significant number of sources explore the benefits of community-led responses aimed toward reforming or sensitising external factors such as the police. This ranges from formal training of individual police officers, healthcare providers and other public officials to the creation of institutional relationships. Positive benefits include reductions in police violence and, resultingly, safer sex practices and better access to services.
Case Study 2 — Organisational development in six Indian districts. A 2016 study analysing the impact of community-led organizations in six districts in India found that a focus on strengthening the community-led interventions in terms of organisational development helps overcome several barriers by community collectivization. This translates into reduction in financial vulnerability by reduced chances of exploitation by law enforcement agencies and improving access to microfinance and, thereby, reducing reliance on exploitative lending sources. The community-led initiatives have the ability to improve not only the health outcomes but also the social determinants of health.
Another means of shifting practices and implementation described in the sources are community-led monitoring, observation and other forms of accountability focused on the gap between the experience of community members and the commitments in law, policy and human rights. Beyond implementation, community-led responses can also be effective in reforming law and policy. Such efforts include publication of advocacy tools, direct lobbying with policymakers and officials, protests and advocacy to counter government-led messaging.
Case Study 3 — New Zealand Prostitutes Collective (NZPC). An example of a community-led response for improving the legal determinants of sexual and reproductive health can be seen in a sex worker-led response in favour of harm reduction and law reform advanced by the New Zealand Prostitutes Collective (NZPC) that resulted in the country’s decriminalisation of sex work. From its founding, the NZPC was caught between a police force that was seeking to enforce criminalising laws and a Ministry of Health that funded the organisation to provide certain health promoting and harm reduction services. Eventually, following agitation by NZPC, the broader community and other allies, legislation decriminalising sex work was passed. This law removed an obstacle to NZPC’s responses for community health, enabled sex worker collectivisation and promoted further community involvement in shaping policy on health. This case is an example of how community-led responses can shift the legal determinants of sexual and reproductive health and rights by promoting law reform and helping shape its implementation.
Regarding health outcomes
Community-led responses for HIV and broader sexual and reproductive health have both direct and indirect impacts on the health and well-being of key and vulnerable populations. The Review found numerous benefits attributed to or associated with community-led responses including increased HIV diagnoses, PrEP initiation and access to antiretroviral therapy. Among the most frequently cited benefits in the sources is an increase in condom use, which is often directly associated with a decrease in sexually transmitted infection prevalence or incidence. Related benefits include increased health, reduced psychological distress, better referral to psychological services. Community-led services are shown providing harm reduction, maternal health, and family planning services.
For example, community-led crises response intervention in South Africa focused attention on gender-based violence among female sex workers and, despite being underfunded, it was able to increase access to health and psychosocial services. Similarly, the “Wired program” in Australia addressed the higher use of methamphetamine among men who have sex with men living with HIV — up to 30% as compared to 2% in the general population. Community-led responses also found success by delivering programming at the intersection of HIV and broader sexual and reproductive health services. For instance, a Community Randomized Control Trial in Tanzania linked structural violence, family planning services and pregnancy with HIV prevention services for female sex workers.
The value of better legal environments
Regarding community leadership
Positive laws, policies and practices promote community-led responses and ally civil society organisations by directly recognising them and by lifting direct and indirect barriers to their operations. Legal recognition broadly encompasses activities by policymakers and officials that positively benefit community-led and civil society organisations. One form of recognition seen in the sources is the accordance of legal status to activities, such as harm reduction or testing services, undertaken within community-led responses. Recognition also includes certain forms of legal personality to community-led organisations or government’s creation of partnerships with communities of key and vulnerable populations. Another is providing dedicated funding for needed services, such as harm reduction, and capacity building among community-led and community-based organisations.
Case Study 4 — Stigma and sex-work decriminalisation across three countries. An analysis amalgamated the findings of eight projects in three countries to highlight the impact of community interventions for addressing HIV. It elucidates how, at the global level, persistent stigma and discrimination leads to perpetuation of regressive international laws and policies and funding constraints for community-led interventions. At national level, it highlights how negative legal determinants lead to a vicious cycle wherein laws criminalizing sex work hamper the ability of sex workers to organize and increase stigma, discrimination, and violence among sex workers. It also highlights how a shift towards breaking these barriers, which in this case is decriminalizing sex work, helps build social cohesion and ensure community empowerment.
The sources describe how community-led responses and the work of ally civil society organisations can be enabled by anti-discrimination measures as well as decriminalisation and legalisation of, respectively, sex work and drug harm reduction services.
Case Study 5 — New Zealand National Needle Exchange and DIVO. A law that both recognised community-led organisations and removed a barrier to community-led responses can be seen in the initiative for New Zealand’s national needle exchange programme. The initiative to recognise the harm reduction service came in response to activism and existing practices in the grey zone of the law. The legislation itself legalised and funded the provision of needles and syringes via local organisations led by people who inject drugs that could apply for recognition. One of these organisations, the Dunedin Intravenous Organisation (DIVO), not only provided the service it was contracted for by the government but also went beyond it to conduct and participate in research, form cross-organisation ties, present at conferences, publish community literature, and build up community capacity. In this way, the source presents a positive feedback loop of community-led response leading to law reform that, in turn, promoted yet more community-led responses.
Another way of seeing the benefits that positive legal environments have for community-led responses is by seeing the impediments presented by negative laws, policies and practices which can and do frustrate community leadership and ally civil society. Some of the most common barriers are laws and policies that directly prohibit or burden community-led organisations and ally civil society organisations. Prohibition and non-recognition are frequently deeply entangled with the criminalising, discriminatory and punitive laws and policies applied towards members of key and vulnerable populations.
Case Study 6 — Silver Rose and CSO non-recognition (Arps & Golichenko). An example of the negative impacts of non-recognition of a civil society organisation can be seen in a study by Arps and Golichenko concerning a community-led response aimed at benefiting sex workers, helping prevent HIV, and working towards better sexual and reproductive health. To better perform these activities, they needed legal recognition of their CSO, Silver Rose, since this would grant access to financing, the courts, and other benefits. The application was declined due to a discriminatory administrative determination connected with the punitive ban on sex work. As a result of only being allowed unregistered association, their purposes of providing education and information for sex workers, promoting safer and healthier work practices, and offering legal help and conflict resolution were frustrated.
Related to these more direct forms of prohibition and non-recognition are the indirect barriers created by generally applicable laws and policies designed with paternalism toward or lack of regard for the needs of key and vulnerable populations. Examples include the structuring of funding application criteria and processes toward actors with more resources and capacity than community-led organisations typically have.
Case Study 7 — “Anti-drug drive operations” in Dhaka. In Dhaka, “anti-drug drive operations” not only caused harm directly to people who use drugs by causing police to engage in extrajudicial violence and provoking risk injection practices but also frustrated community-led responses by exposing outreach workers to police violence and obstructions as well as by dispersing those they were seeking to help.
Criminalising, discriminatory and punitive legal environments pose barriers to community-led responses and can erode or inhibit community capacity. Less direct impacts can flow on from the discourse and stigma produced by criminalisation in institutional distrust from affected communities that prevents or undermines their cooperation with official actors, including healthcare providers.
Case Study 8 — GROOTS Kenya and property rights. An example of how legal environments impact community-led responses in diverse ways can be seen in the successful community-led response by GROOTS in Kenya aimed at protecting vulnerable women and responding to HIV by upholding property rights. This initiative was partly frustrated by fragmented land laws and a lack of integration between community-led mechanisms for securing land tenure and the formal legal system. This shows that those laws, policies and practices which undermine community-led responses will not always be criminalising or outright discriminatory.
Regarding health outcomes
The literature relevant to HIV identified within the Review encompasses sources that describe numerous benefits of improved legal determinants and harms of negative legal determinants to sexual and reproductive health.
For one specific issue — sex work decriminalisation — benefits are identified such as measurable increases in safe sex practices, declines in gender-based violence, and reductions in the incidence of HIV and sexually transmitted infection. In particular, decriminalisation is identified with better control over work, access to social services and protection against exploitation, harassment and violence. One study quantifies the economic benefits of decriminalisation in terms of income generated for the sex workers per year and in terms of savings for the criminal justice system and the health system.
Among the most commonly described direct costs of negative laws, policies and practices is the effect that criminalisation and discrimination have on utilisation of and access to health services, including preventive and harm reduction services. Various negative laws, policies and practices, most prominently criminalisation, are also more directly associated with reduced availability, accessibility and adoption of harm reduction services and practices. Gender-based and other interpersonal violence is also a product of negative laws, policies and practices as well as an important social determinant of health.
Deep Dive 2 — The Limits to Law Reform. Law reform that does not centre communities or their needs needs to be avoided. Coercive laws purportedly aimed at improving health not only contradict rights but often also either subvert or fail to achieve their objective. For example, Canadian laws criminalising HIV non-disclosure were intended for promoting prevention but instead exacerbated transmission rates while also disproportionately affecting already marginalised people and women. Similarly, in the Canadian province of British Columbia, non-criminalisation of sex work alone was not sufficient for improving either health or protecting rights when the broader legal environment remained hostile to the labour rights and business practices of sex workers. Legislative reform is not, itself, always enough when the rights, needs and leadership of affected communities are not centred in the reform’s design. Moreover, even when the primary legal initiative is well designed it may require other supportive policies and practices to ensure its intended effect.
The resourcing of community-led responses
Reliance on community resources
One of the major resources available to community-led responses is the labour, creativity and, in some cases, resources of the community members themselves. Despite the benefits to the broader community and society that result from these efforts, volunteers are often unpaid, underpaid and uncompensated. When there is payment, we often see workers being paid wages while volunteers are paid small fees or inducements — although even in these cases it is unclear whether the level of remuneration is appropriate or sufficient.
The reliance of many community-led responses on the time, money and other resources of volunteers can be both a strength and weakness. Various questions are raised as to the sustainability and limitations of leaving crucially needed volunteers unpaid, underpaid and under-resourced. Despite this, the situation in which community volunteers remain unpaid or underpaid and, in many cases, provide financial support to the response is even more left unquestioned. When it is interrogated, reliance on unpaid or underpaid volunteers has also been identified as a cost-saving advantage of community-led responses. One study notes how “unpaid volunteers alone add an estimated 56 percent, on average, to CBO [community based organisation] budgets in Kenya, Nigeria, and Zimbabwe”.
Fair wages could help further advance the commitment of the community towards their community-led responses. To ensure fair wages, however, community-led organisations need to be well-resourced. Accordingly, it is up to national and other funders to close the gap through their own investment in community-led responses.
Evidence as to the adequacy and scale of investment
Aside from the voluntary contributions of community members, sources of funding and resources for community-led responses identified in the Review varied with the main categories being government, donors and user fees. Limitations in the amount and certainty of this funding, as well as the conditions attached to the use of available funds, are identified as a major problem and challenge for community-led responses.
Examples include community-led organisations shuttering or reducing programmes due to insufficient and uncertain funding. A related issue arises when funding is limited to narrow vertical interventions by government or as part of donor-driven priorities, where community priorities are underfunded and overall community capacity building is under-resourced. Funding interruptions and shifts in governance arrangements are also identified as causes for community ownership over responses either failing to eventuate or degrading.
The particular need for scale and long-term investment is acute in the case of community-led responses that often will require capacity building to realise the advantages of co-creation and scale to maximise cost-effectiveness. Despite this, relatively few interventions covered within the Review were accompanied by capacity or implemented at scale.
Underpinning the 30-80-60 targets on community leadership in the HIV response was the commitment to ensure the sustainable financing of community-led organisations and networks. Given that community-led responses are being impeded and burdened by funding and resourcing issues, delivery on this commitment is urgently needed.
Description of the types of resourcing received
Specific figures, evaluations and estimates for sources encompassed by the Review vary substantially. For instance, according to one study, the positive impact of community-led interventions stems from three factors: community ownership helps in understanding the unmet needs and thereby designing a better program and implementation strategy; it is cheaper as the community members are ready to work voluntarily (spending US$1.5 per person helped per year, much lower than most interventions); and the focus on reducing structural impediments and vulnerabilities. In this case the intervention aimed at improving the ability to negotiate condom usage by enhancing financial security of female sex workers via self-help groups.
Another study highlights the importance of scale and time in understanding the impact of community-led interventions. A cluster-randomised trial comparing community-led distribution of HIV self-testing kits against community-based distribution by paid distributors in 40 rural Zimbabwean communities cited costs of $285,065 with 46% of this being human resources, 23% for HIV self-testing kits and 8% for vehicles. The professionally supervised paid distributor model was more expensive than the community-led model and witnessed improvement in efficiency and costs over time and with scaling up.
Deep Dive 3 — Gaps in Monitoring. Despite diverse findings associating the responses with various benefits, there is an absence in the included literature on the current share of services and programmes delivered as part of community-led responses both globally and in individual countries. This is a glaring issue given that the quantitative targets in the Global AIDS Strategy specifically require that, by 2025, 30% of testing and treatment, 80% of prevention and 60% of societal enabler programming are to be delivered by communities globally and within countries. UNAIDS estimates that across countries with available data for 2019–2021, key populations-led organizations reached 40% of sex workers, 31% of gay men and other men who have sex with men, 26% of people who inject drugs and 37% of transgender people with prevention interventions. A systemic issue is that studies, implementers, and funders do not accurately distinguish or commonly disaggregate in publicly available information between community-based interventions and community-led interventions. To begin addressing this gap, UNAIDS announced in mid-2022 that it was planning to systematically monitor investments in and expenditures by community-led organisations as a way of tracking and motivating progress toward the realisation of the 30-80-60 targets.
Key recommendations
1. The Review supports the need to view progress on community-leadership and societal enablers — in particular legal determinants — as inseparable and can substantiate arguments in favour of investment in each and both. There is a mutually reinforcing interrelationship between improving community leadership and realisation of progress on the societal enablers, including legal determinants. By acting on both aspects at the same time with elevated and higher-quality investment, a mutually reinforcing cycle of improvements in the conditions for community-led responses and legal and societal environments conducive of improved sexual and reproductive health and rights will be triggered.
2. The Review supports the argument that legal environments which undermine health and community-led responses need to be reformed urgently with broad changes to laws, policies and practices that target all forms of criminalisation, discrimination and marginalisation. Addressing the harms of criminalisation and other negative laws and implementing laws to protect against discrimination and decriminalise people and their behaviours is urgent. At the same time, isolated reforms which target only a single component of complex and intersectional forms of legal, extra-legal and societal marginalisation and discrimination can be of limited effect. In the absence of action, health is harmed, health services impaired and the community-led responses are obstructed and frustrated.
3. The Review can be cited to support investment in and advocacy for high-ownership community-led responses to HIV and related sexual and reproductive health challenges. Community-led responses benefit health and they are shown to have impact in delivering health services, ensuring prevention and moving the needle on critical legal determinants and related societal enablers. Community ownership also benefits the prioritisation and design of responses by ensuring they target areas of greater community need and, in particular, grapple with the challenges posed by preventing, mitigating and reforming bad laws. Global and national responses that aim to meet the challenge of HIV with sufficient ambition thus need to have community leadership at their heart and promote the highest level of community ownership attainable.
4. The Review’s findings can be used to substantiate the need for and benefits of increased investment in the capacities and responses of community-led organisations that is both predictable and not burdened by conditions. Community-led responses are undermined by uncertain and inadequate funding. These funding challenges make delivering the services or programming needed challenging, difficult or impossible. More subtly, they can also warp the character of the community-led response by requiring communities to fit the prescriptions and reporting requirements of funders rather than the needs and processes preferred and most suited to the communities themselves. High-quality and high-ownership community-led responses require capacitation and organisational development over the long-term which makes sustained and predictable funding essential. There is a pressing need to hold countries and funders to account in fulfilling this commitment.
5. The Review finds an overreliance on community members to volunteer their time, labour and resources to the responses they lead and recommends compensating them instead. Shifting funding and programming to community-led responses as a means of exploiting their passion to extract free labour and other resource commitments from already marginalised populations is wrong and the overreliance on community volunteerism should be reduced. The benefits of community leadership should, instead, be located in the “leadership” of the communities: the immense added value of directing resources to people who know their needs and their capacities can innovatively advance responses to HIV and related sexual and reproductive health challenges. Community-led organisations need to be resourced well enough so that roles which merit compensation and wages should receive them.
For more recommendations on policy change and research, please see the full Review.